1.1 Historical Perspective of Intellectual Disability (ID)
Pre-Colonial India
Historically, over different periods of time and almost till the advent of the colonial rule in India, including the reigns of Muslim kings, the rulers exemplified as protectors, establishing charity homes to feed, clothe and care for the destitute persons with disabilities. The community with its governance through local elected bodies, the Panchayati system of those times, collected sufficient data on persons with disabilities for provision of services, though based on the philosophy of charity. With the establishment of the colonial rule in India, changes became noticeable on the type of care and management received by the persons with the influence from the West.
Pre-Independence–Changing Life Styles in India
Changes in attitudes towards persons with disabilities also came to about with city life. The administrative authorities began showing interest in providing a formal education system for persons with disabilities, particularly for families which had taken up residences in the cities.
Changes in the lifestyle of the persons with mental retardation were also noticed with their shifting from ‘community inclusive settings’ in which families rendered services to that of services provided in ‘asylums’, run by governmental or non-governmental agencies (Chennai, then Madras, Lunatic Asylum, 1841).
It was at the Madras Lunatic Asylum, renamed the Institute of Mental Health, that persons with mental illness and those with mental retardation were segregated and given appropriate treatment.
Special schools were started for those who could not meet the demands of the mainstream schools (Kurseong, 1918; Travancore, 1931; Chennai, 1938). The first residential home for persons with mental retardation was established in Mumbai, then Bombay (Children Aid Society, Mankhurd, 1941) followed by the establishment of a special school in 1944. Subsequently, 11 more centres were established in other parts of India.
![]()
![]() Post-Independent
India–Current Scenario
Post-Independent
India–Current Scenario
Establishment of Special Schools
Article 41of the Constitution of India (1950) embodied in its clause the “Right to Free and Compulsory Education for All Children up to Age 14 years”.
Many more schools for persons with mental retardation were established including an integrated school in Mumbai (Sushila Ben, 1955).
Notwithstanding this obligatory clause on children’s mainstream education, more and more special schools were also being set up by non-governmental organizations (NGOs) in an attempt to meet the parents’ demands.
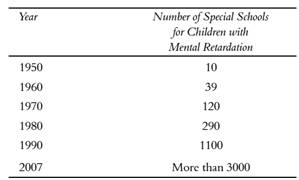
Special Schools
Establishment of special schools in the country since independence is shown below
Indian Education Commission, 1964-66
![]()
![]()
The Indian Education Commission, 1964-66 made a clear mention of the presence of only 27 schools for persons with mental retardation in the entire country at that time.
In 1953, training teachers to teach persons with mental retardation was initiated in Mumbai by Mrs. Vakil.
In 1971, special education to train persons with mental retardation was introduced in Chennai at the Bala Vihar Training School by Mrs. M. Clubwala Jadhav.
In the same year, the Dilkush Special School was established in Mumbai initiating special teachers’ training programs.
The various Acts passed and the policies touching the lives of the disabled are dealt with in Chapter 11, Policies and Programmes.
1.2 Definitions of Intellectual Disability – ICD-10, AAIDD, WHO, PwD Act 1995, RPD bill (Proposed), DSM (Latest)
WHO, ICD-10- Mental retardation is a condition of arrested or incomplete development of the mind, which is especially characterized by impairment of skills manifested during the developmental period, that contribute to cognitive (knowledge), language, motor and social abilities.
AAIDD, 2010- Intellectual disability is a disability characterized by significant limitations both in intellectual functioning and in adaptive behavior, which covers many everyday social and practical skills. This disability originates before the age of 18.
PWD Act, 1995- Mental retardation means a condition of arrested or incomplete development of mind of a person which is specially characterized by sub normality of intelligence.
RPwD Act 2016- Intellectual disability is a condition of arrested or incomplete development of mind of a person, especially characterized by sub-normality of intelligence.
DSM-5 defines intellectual disabilities as neurodevelopmental disorders that begin in childhood and are characterized by intellectual difficulties as well as difficulties in conceptual, social, and practical areas of living. The DSM-5 diagnosis of ID requires the satisfaction of three criteria:
· Deficits in intellectual functioning—“reasoning, problem solving, planning, abstract thinking, judgment, academic learning, and learning from experience”—confirmed by clinical evaluation and individualized standard IQ testing;
· Deficits in adaptive functioning that significantly hamper conforming to developmental and socio-cultural standards for the individual's independence and ability to meet their social responsibility; and
· The onset of these deficits during childhood.
1.3 Etiology Causes and Prevention
Causes of Intellectual Disability
Possible Sources for Causes of Intellectual Disability:
Prenatal (before birth)
– chromosomal, maternal infections, environmental factors, unknown influences
Perinatal (during birth)
– gestational disorders, neonatal complications
Postnatal (after birth)
– infections and intoxicants, environmental factors
Predisposing Factors
§ No clear etiology can be found in about 75% of those with Mild MR and 30 – 40% of those with severe impairment
§ Specific etiologies are most often found in those with Severe and Profound MR
§ No familial pattern (although certain illnesses resulting in MR may be heritable)
Heredity (5% of cases)
– Autosomal recessive inborn errors of metabolism (e.g., Tay-Sachs, PKU)
– Single-gene abnormalities with Mendelian inheritance and variable expression (e.g., tuberous sclerosis)
– Chromosomal aberrations (e.g., Fragile X)
§ Early Alterations of Embryonic Development (30% of cases)
– Chromosomal changes (e.g., Downs)
– Prenatal damage due to toxins (e.g., maternal EtOH consumption, infections)
§ Environmental Influences (15-20% of cases)
– Deprivation of nurturance, social/linguistic and other stimulation
§ Mental Disorders
– Autism & other PDDs
§ Pregnancy & Perinatal Problems (10% of cases)
– Fetal malnutrition, prematurity, hypoxia, viral and other infections, trauma
§ General Medical Conditions Acquired in Infancy or Childhood (5% of cases)
– Infections, trauma, poisoning (e.g., lead)
The following table summaries the causes of Intellectual Disability:

Etiology
– At least 500 causes now known
– Over 150 MR syndromes have been related to the X-chromosome
– Most common cause of MR:
1. Down’s Syndrome (most common genetic cause)
2. Fragile X Syndrome (accounts for 40% of all X-linked syndromes; most common inherited cause)
3. Fetal EtOH Syndrome (most common attributable cause)
4. together these 3 account for 30% of all identified cases of MR
Prevention
Prevention refers to the measures taken to prevent the disability from occurring.
The World Health Organisation (WHO), American Association for Mental Retardation (AAMR), American Association on Mental Deficiency (AAMD), International Classificatioon on Deficiency (ICD), Diagnostic and Statistical Manual (DSM-IV) definitions of mental retardation relate to three levels of prevention:
· Primary level of prevention is carried out by doctors and health professionals to prevent manifestation of the disability.
· Secondary level prevents the manifestations of additional disabilities and regression.
· Tertiary level mitigates the impact of disability on social isolation, stigmatization of the handicap.
Based on the principles of early identification and intervention, prevention of mental retardation is taken as early as possible.
Prenatal Prevention relates to
· Dealing with causal factors such as Rh incompatibility; maternal illness, infections and other high risk conditions, such as malnutrition in mother and child during the first trimester of pregnancy, environmental and occupational hazards and consanguinity.
· Prenatal diagnosis where preliminary investigations are carried out, blood and urine tests investigations to assess the foetal abnormalities through ultra sonography, radiography, and aminocentesis.
· Immunization to the mother for preventing illnesses and infections leading to disability in the foetus.
· Follow up action is provided through periodic checkups, prompt treatment and effective management plan with a balanced diet and periodic health checkups.
Natal Prevention relates to
· Delivery conducted under hygienic conditions by a trained person and/or in a hospital, to prevent breech delivery, asphyxia, prematurity with low birth weight, occurrence of jaundice, and other post-illnesses in the child.
· Care of new borns at high risk for mental retardation in well equipped neonatal intensive care units; a close follow up to identify delays and abnormalities in development; facilitating interventions and corrections at the earliest thereby reducing the severity of handicap.
Postnatal Prevention relates to
· Neonatal screening with simple blood and urine tests for metabolic abnormalities and hypothyrodisim, associated conditions that lead to mental retardation.
1.4 Classification – Medical, Psychological, Educational (Recent) and ICF
Medical classification
1. Infections and intoxications
2. Trauma or physical agent
3. Metabolic or nutrition
4. Gross brain disease (post natal)
5. Unknown prenatal influence
6. Chromosomal abnormality
7. Gestational disorders
8. Psychiatric disorder
9. Environmental influences
10. Other influences
Psychological classification
Based on the 1983 AAMR definition, the operational classification for persons with mental retardation is as follows:

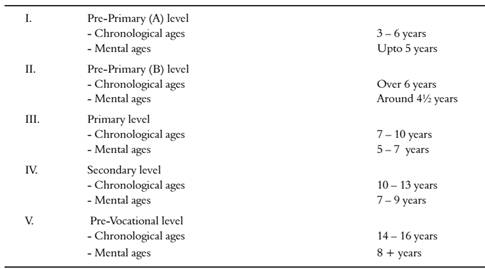
Educational Classification
In the special education centers in India, the classroom classification in operation is as shown below:
AAMR Levels of Support
Intermittent - Support is not always needed. It is provided on an "as needed" basis and is most likely to be required at life transitions (e.g. moving from school to work .
Limited - Consistent support is required, though not on a daily basis. The support needed is of a non-intensive nature.
Extensive - Regular, daily support is required in at least some environments (e.g. daily home-living support).
Pervasive - Daily extensive support, perhaps of a life-sustaining nature, is required in multiple environments.
1.5 Screening, Identification, Characteristics and Needs of PwID
Screening
· A procedure by which accurately categorizes individuals as possibly handicapped or delayed.
· Primary concern is identification of those for whom more complete diagnostic study (further assessment)is necessary.
· It does not indicate that a person is handicapped or delayed
· Formal and informal observation and frequency counts of observed behavior are frequently used.
Pre-natal procedures
Blood test in the mothers
· Hemoglobin levels
· Glucose level
· VDRL (Venereal Disease Research Laboratory Test)
· Blood group and Rh
· Blood antibody titers for TORCHS
Ultrasonography
· Neural tube defects like microcephaly, hydrocephaly, etc can be identified during II trimester.
· Intra Uterine Growth Retardation
Maternal Serum AFP (Alpha-fetoprotein)
· 16-18 weeks of pregnancy
· Detect spina-bifida, anencephaly, down’s syndrome etc
· Not accurate indicator, only suggests further testing
Chorionic villus sampling
· 7th to 9th week of pregnancy
· It shows chromosomal abnormalities carried by the fetus.
· Tiny piece of chorionic villous tissue from placenta is removed and tested.
Multiple marker screening
· 15th to 20th week of pregnancy
· Screen NTD, trisomy – 21, and trisomy – 18
· Done by a blood test – measures the following
1. hCG (human chorionic gonadotropin), which is made by the placenta
2. estriol, which is made by the placenta and the fetus
3. alpha-fetoprotein (AFP), which is made by the fetus
Amniocentesis
· 16th week
· Detects down’s syndrome, Tay-sachs, sickle cell anemia, and many other genetic disorders
· Women reached 35 yrs of age
· Withdrawal of a sample of fluid surrounding the fetus
· 0.06% chance of miscarriage
Fetoscopy
· A small (3–4 mm) incision is made in the abdomen, and an endoscope is inserted through the abdominal wall and uterus into the amniotic cavity.
Neonatal Screening
APGAR Score
A – Appearance (colour)
P –pulse rate (Heart rate)
G – Gravity (Muscle tone of extremities)
A – Activity (response to catheter)
R – Respiratory effort
Scoring 8 to 10 is normal. Below 7 high risk infant
Urine test for metabolic disorders
Post-natal Screening
Ultrasound
· For intracranial pathology
· Reveals intra cranial hemorrhage, displacement of brain midline structures, pathological cavities.
EEG- electroencephalogram for seizure disorder
Computerised Tomography
· Detects anoxia of tissue, intracranial hemorrhage, hydrocephalous, and congenital anomalies like congenital cysts, calcifications etc.
MRI- Magnetic Resonance Imaging (MRI)
Blood chemical tests in neonatal screening
· Identify metabolic disorders, cretinism
· Tandom mass spectrometry - can screen for more than 20 inherited metabolic disorders with a single drop of blood
· Genetic Counseling
![]()
![]() Other Screening Tools
Other Screening Tools
Some of the other popularly used tools in India include
· Cooperative preschool inventory-Caldwell.
· Croydon Scales (Screening Checklist) (Wolfendale & Bryans).
· Denver Developmental Screening Test (Frankensberg, Dodds and Fandal).
· Early Childhood Assessment: A criterion referenced screening device (Schmaltz, Schramn and Wendt).
· AGS Early Screening Profiles (Harrison, et al.).
· Developmental Indicators for the Assessment of Learning-R (Mardell, et al.).
· Early Screening Inventory (Merisels, et al.).
· Brigance ‘K’ and ‘T’ Screen for Kindergarten and First Grade (Brigance).
Indian Screening Tools
· Developmental Screening Test (DST) by Bharat Raj is a widely used screening tool by professionals. The NIMH schedules noted earlier are used for further referral.
· Upanayan Early Intervention Programming System (1987).
· Functional Assessment Check List for Programming (FACP) 1991.
· The revised Madras Developmental Programme System Behavioural Scale MDPS-A curriculum based assessment checklist (1975) is suitable for identification purposes.
Characteristics of Intellectual Disability
Mild ID Profile
· Minor delays in the preschool period
· Evaluation often only after school entry
· 2-3 word sentences used in early primary grades
· Expressive language improvement with time
· Reading/math skills – 1st to 6th grade levels
· Social interests typically age appropriate
· Mental age range of 8-11 years of age
· Persistent low academic skill attainment can limit vocational possibilities
Moderate ID Profile
· More evident and consistent delays in milestones
· At school entry may communicate with single words and gestures
· Functional language is the goal
· School entry self-care skills – 2-3 year range
· By age 14: basic self-care skills, simple conversations, and cooperative social interactions
· Mental age of 6-8 years of age
· Vocational opportunities limited to unskilled work with direct supervision and assistance
Severe ID Profile
· Identification in infancy to two years
· Often co-occurring with biological anomalies
· Increased risk for motor disorders and epilepsy
· By age 12: may use 2-3 word phrases
· Mental age typically 4-6 years of age
· As adults assistance typically required for even self-care activities
· Close supervision needed for all vocational tasks
Profound ID Profile
· Identification in infancy
· Marked delays and biological anomalies
· Preschool age range may function as a 1-year-old
· High rate of early mortality
· By age 10: some walk/acquire some self-care skills with assistance
· Gesture communication
· Recognizes some familiar people
· Mental age range from birth to 4 years of age
· Functional skill acquisition not likely
Supports and Support Needs
There is a reciprocal relationship between intensity of support needed and extent of limitations in personal competency. There are, however, many influences on support needs that are not associated with aspects of personal competence that have been traditionally aligned with measuring impairments to intellectual functioning. For instance, the presence of health problems/medical conditions, limitations in physical strength, stamina and mobility, and challenging behaviors significantly impact the nature and intensity of support that a person requires to participate in culturally valued settings and activities.
Thompson et al. (2009) defined support needs as “a psychological construct referring to the pattern and intensity of supports necessary for a person to participate in activities linked with normative human functioning”. Like other psychological constructs, the intensity of a person’s support needs (just as the intensity of someone’s motivation, courage or shyness) must be inferred because it is not directly observable. Over the past 15 years, several new assessment scales have been introduced that purport to measure support needs. The most widely used assessment tool is the Supports Intensity Scale of which there is an Adult Version and Children’s Version. Both versions are unique among support needs assessment scales because they generate norm-referenced, standard scores upon completion.
Individualized Supports
Individualized supports are “resources and strategies that aim to promote the development, education, interests and personal well-being of a person and enhance individual functioning”. Specialized instruction is one class of support. Years of research have produced evidence for effective strategies to teach a person new skills to enhance their personal competency, and thus bridge the person-environment gap. Technology is another class of supports, enabling people to function more competently and efficiently. There are also a wide range of supports designed to modify or adapt the environment. Again, the critical feature of supports is that they bridge the gap between limitations in personal functioning and environmental demands. Therefore, anything that increases the capacity of the environment to fully include a person (i.e., mitigates the demands of settings or activities) is as much of a support as something that increases the competency of the person. Lowering file cabinets for an office worker who uses a wheelchair is an example of an environmental accommodation (the environment has been adapted so the office worker can do the job), as is allowing a student who does not have strong reading skills to take a multiple choice history exam orally. The environment for testing has been changed to allow the child to demonstrate knowledge of historical information covered on the test.