Unit 1: Listening Devices and Classroom Acoustics
1.1 Listening devices: Types (Individual & Group), functioning of Hearing aids, classification of hearing aids based on style (body level, ear level), technology (analog, programmable, digital), Ling’s six sound test and other outcome measures
1.2 Ear moulds: Types, Importance, Care & maintenance
1.3 Classroom amplification devices: Individual, Speech Trainer & group, Hard wire, loop induction, infra-red & FM systems, their importance in educational management
1.4 Cochlear Implant, middle ear implant, BAHA & Auditory Brainstem implant: Candidacy, components, functioning & importance with special reference to ADIP 2014 scheme
1.5 Comparison between individual hearing aids, group hearing aids & cochlear implant and their care & maintenance
1.1 Listening devices: Types (Individual & Group), functioning of Hearing aids, classification of hearing aids based on style (body level, ear level), technology (analog, programmable, digital), Ling’s six sound test and other outcome measures
Listening devices are used for hearing impaired individuals to compensate for their hearing loss. These devices aim at making all sounds available in the environment as well as speech of others, audible and clear for hearing impaired individuals. These devices are available in a variety of types depending on style, size, capacity (power) and technology. There are many makes/brands available commercially which vary in price range again depending on the above mentioned types.
In some situations amplification device (such as hearing aids, Cochlear implants etc) is not sufficient alone. In such cases these devices are paired with Assistive Listening Devices. Assistive Listening Devices (ALD) can be worn separately or paired with the amplification device. E.g FM system, Loop induction system etc
Another very important classification is based on the place of stimulation done by the respective devices. The device can deliver amplified sounds directly to the external ear, or directly to the hearing nerve, or directly to the mastoid bone (bone behind external ear).
Listening devices again can be broadly classified as
1) Hearing Aids
2) Cochlear Implants
3) Middle Ear Implants
4) Bone Anchored Hearing Aids
5) Auditory Brainstem Implants.
INDIVIDUAL VS GROUP LISTENING DEVICE
INDIVIDUAL LISTENING DEVICE – This type is useful for one individual at a time. It is a called a personalized device. The speech and other sounds are picked up by the device and delivered to the individual wearing it. The amplification device (hearing aid or cochlear implant) has a microphone on its surface to pick up sounds/speech, which is amplified inside the device and then delivered directly to the individual’s hearing system. The individual can carry it with him/her. It is totally wearable and portable. Assistive listening device also can be individual in nature e.g FM system which can be paired with individual hearing aid.
GROUP LISTENING DEVICE - As the name suggests this system aims to help a group of hearing impaired individuals at the same time with a common device. This arrangement is usually used in a special classroom. The teacher has a microphone which picks up the teacher’s voice, which is then amplified and sent to headphones/receivers worn by multiple students. So the teacher’s voice is heard clearly by a group of students.
Assistive Listening Devices such as loop induction system can also be installed in large areas like classrooms where a loop is installed across the room. The sounds picked up by the microphone are transformed and run through the loop. The telecoil of the hearing aids worn by individuals picks up the signal and it is heard by the individual.
The terms assistive device or assistive technology can refer to any device that helps a person with hearing loss or a voice, speech, or language disorder to communicate. These terms often refer to devices that help a person to hear and understand what is being said more clearly or to express thoughts more easily. With the development of digital and wireless technologies, more and more devices are becoming available to help people with hearing, voice, speech, and language disorders communicate more meaningfully and participate more fully in their daily lives.
Health professionals use a variety of names to describe assistive devices:
- Assistive listening devices (ALDs) help amplify the sounds you want to hear, especially where there’s a lot of background noise. ALDs can be used with a hearing aid or cochlear implant to help a wearer hear certain sounds better.
- Augmentative and alternative communication (AAC) devices help people with communication disorders to express themselves. These devices can range from a simple picture board to a computer program that synthesizes speech from text.
- Alerting devices connect to a doorbell, telephone, or alarm that emits a loud sound or blinking light to let someone with hearing loss know that an event is taking place.
Functioning of Hearing aids
Before understanding the basic working of a hearing aid, it is essential to know the parts of a hearing aid. The basic parts are as follows:
1) Microphone
2) Amplifier
3) Receiver
4) Telecoil
5) Volume Control
6) Tone Control
7) On/Off switch
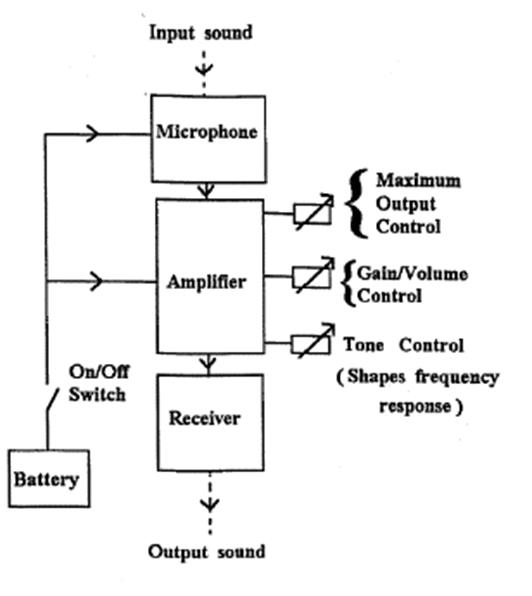
The microphone picks up sounds around it and sends to the amplifier, where the sounds are amplified and filtered in many ways and then finally sent to the receiver which is worn by the hearing impaired individual in his external ear. The hearing aid is powered by a battery. The electronic components consist of transducers, capacitors, resistors, transistors, printed circuit boards are used. An electromagnetic coil system is used to make the telecoil , which helps to hear telephone conversation, speech in induction loop systems etc.
CLASSIFICATION OF HEARING AIDS
BASED ON STYLE
The earliest of amplification system were very basic, non electronic models like ear horns, trumpets etc. Research and development led to the first electric hearing aids which gradually improvised in style and size in order to satisfy the technological advancements as well as cosmetic preference of users. Hearing impaired individuals mostly wanted hidden hearing aids so the miniaturization of size was gradually developed in hearing aid industry.
1) Body level hearing aids – As the name suggests the hearing aid is worn on the body of the hearing impaired person(e.g. in the pocket/blouse). The body of the hearing aid has a cord which connects to a receiver, which looks like a button and worn in the ear of the hearing impaired person.

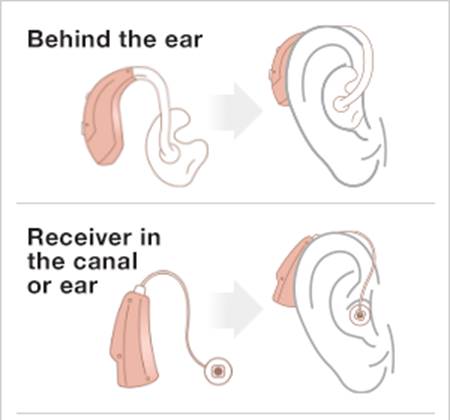
2) Behind the ear type – These hearing aids are wearable over the pinna or behind the external ear. The basic parts inside the hearing aid are similar to body level hearing aid only miniaturized in size and advanced technology. The whole hearing aid fits behind the ear, the receiver is also housed in the hearing aid case. The amplified sound reaches the ear via a ear mould or ear tip.


3) In the ear hearing aids – These hearing aids are wearable inside the ear, the body of the hearing aid sits in the ear canal with its external part/faceplate sits at the start point of ear canal i.e. concha. As these hearing aids are smaller than the previous two styles, the internal parts are yet more miniaturized and placed closer to each other in the hearing aid case. As a result these hearing aids come with a lower output or capacity as compared with the previous two styles.

4) Completely in the canal hearing aid - This type is even smaller than the previous type and sits deeper inside the ear canal. It’s almost invisible from outside. As it is even smaller, it has the lowest output/capacity among all styles. This type is customized and made according to the shape and size of the ear to be fitted.

5) Receiver in the canal- It looks similar to a miniaturized behind the ear hearing aid. The receiver of the hearing aid sits in the ear canal in a separate case/tip and connected via a slim tube with the rest of the hearing aid. The capacity of the receiver can be changed depending on the hearing loss of the person

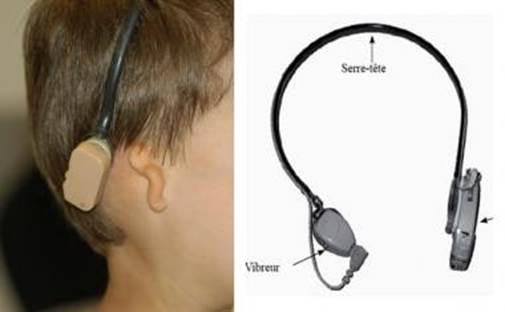
6) Bone Conduction Hearing aid – In some hearing impaired persons conventional hearing aids cannot be fitted. The reason can be malformation of external ear, absence of external ear or a actively discharging ear (presence of pus discharge most of the time due to some active infection in the ear). In these cases a body type hearing aid/behind the ear hearing aid is fitted with a bone conduction receiver, which resembles the one used for bone conduction testing. The bone conduction receiver is placed on the mastoid bone behind the external ear. The amplified sound is transformed into vibrational energy and then delivered to the mastoid bone.


Technology (analog, programmable, digital)
In earlier days the basic technology used in a hearing aid was quiet simple. All the signal/sound picked up by the microphone of the hearing aid was amplified by a common factor without any other alteration. The final sound delivered was just an amplified version of the input sound. However due to limitations of the components inside the hearing aid, the sound was degraded and distorted in most of the cases as it reached the user’s ears. The problem increased when the loudness of the outside sound increased or when the signal was a speech in presence of a background noise. But with the advent of technology the hearing aid industry witnessed a lot of progress within a short span of time. As computer technology advanced, processing speed increased, it was possible to incorporate many features in the hearing aid with less power consumption. Also circuit size could be reduced dramatically.
The technology followed the development path:
Analog- Analog programmable- digital- digitally programmable
ANALOG HEARING AID: These hearing aids continuously make the incoming signal louder. The circuits treat all incoming signal similarly. As the incoming signal becomes louder the analog hearing aid makes it even louder. Some sort of limiting circuits are implemented in the analog circuit, where in the amplifier stops after the incoming signal crosses a particular level of loudness. It is used in body type, behind the ear and even In the ear hearing aids. This technology seems to be helpful for severe to profound losses as compared to lower degrees. Moreover this technology works best for quiet environment. In noisy situations, speech is not clear, as speech and noise are amplified in a similar fashion. This technology will also be helpful for flat hearing losses as compared to sloping hearing losses. Usually the hearing aids using this technology come with simple controls. Other than volume control, there are certain trimmer control options (H N L). Wherein depending upon the slope of hearing loss, low/high frequencies can be emphasized. For flat hearing loss, N (normal) position is the best. Moreover the maximum power output (MPO) can also be adjusted wherein the overall output from the hearing aid can be reduced/increased according to patient’s need. This technology comes with fixed gain and maximum output with minimum adjustments possible
ANALOG PROGRAMMABLE: With the development in computer technology, hearing aids could be designed with a memory. The hearing aids could be programmed in different ways and the two or three programs could be stored and retrieved from memory. The programs can be two different settings in the same hearing aid. e.g one program for indoors and one for outdoors.
DIGITAL HEARING AIDS:
Even more advancements in computer technology led to the advent of digital signal processors. Digital Signal Processors were used in hearing aids. This enabled the hearing aids to convert the input signal/incoming signal, picked by the microphone into digital signals (binary digits). This resulted in faster and much better processing i.e, the output was much better in quality and a better representation of the input signal (original sound). Many studies have shown that in the same group of persons with hearing loss, performance was much better with digital hearing aids than analog hearing aids. Special mention is the performance in challenging situations like in presence of background noise, performance with digital hearing aids is way ahead of analog hearing aids. With the digital hearing aids, the amount of amplification depended on the level of input signal. So for a soft sound, more amplification was given whereas for a loud sound very little or no amplification was given.
DIGITALLY PROGRAMMABLE HEARING AIDS: This Variety of digital hearing aids could be computer programmed. The hearing aid has multiple memories, in which different programs can be stored. The user can change the programs according to specific needs, either with a tiny switch on the hearing aid or with remote control. These hearing aids can be programmed with the help of certain software, which are unique to various manufacturing houses. The hearing aid is connected to the computer via a programming interface. Special adaptors and cables are used for this purpose. Recently the whole arrangement could be made wireless, reducing the need of cables.
These hearing aids come in a variety of capacities, with minimum features to ample features including noise reduction strategy, feedback cancellation, and special treatment to sudden, loud sounds, enhancement of soft sounds, special treatment to speech sounds etc. The price range differs depending on capacity. This type of hearing aids is contemporary, with most of the hearing impaired population fitted with this type. These are also available and approved by Govt.of India, under the ADIP scheme.
OUTCOME MEASURES
The performance with hearing aids needs to be evaluated irrespective of style and technology. The post fitting evaluation is done to understand how much actual benefit the user is receiving with the newly fitted aids. From infants to elder hearing impaired individuals, this assessment is mandatory. The fitting process completes after getting the results with hearing aid.
Certain outcome measures are employed to assess the benefit from hearing aids. These can be questionnaires, aided speech perception tests, aided audiogram, aided behavioral assessment. another handy and quick assessment tool is Ling sounds in Ling’s 6 sound test.
1. Ling’s six sound test
The Ling Six Sound Check is an easy-to-use tool that evaluates how well children are hearing with their cochlear implant and/or hearing aid. The test is a behavioral listening check that uses simple sounds to detect changes in the quality of a child’s hearing. The test should be completed at the start of each school day or therapy session and any time you suspect a child is not hearing as well as they normally do. The sounds used for the Ling Six Sound Check are “ahh”, “eee”, “ooo”, “mmm”, “shh”, and “sss”. These sounds approximately cover sounds ranging from 250-4000 Hz and represent speech in the low, mid, and high frequencies. The chart below describes how these sounds broadly represent the sounds needed to hear spoken language.

The Ling Six Sound Check can be used with children of different ages and various auditory skill levels. Babies and very young children will provide responses that allow you to confirm detection and possibly discrimination. Older children will provide responses that allow you to confirm identification. Keep in mind that a child who is a new recipient of a cochlear implant or hearing aid will begin with detection tasks and then progress to discrimination and identification tasks as appropriate. Below is a description of the auditory skill levels you can test with the Ling Six Sound Check:

Babies (Detection Task) When babies hear one of the Ling Six Sounds presented, they may respond through a behavioral cue such as eye widening, turning their head, or displaying a change in sucking behavior if using a pacifier or having a bottle. Keep in mind the baby must be able to consistently repeat these types of behavioral responses when sound is presented for the response to be considered valid.
Very Young Children (Detection Task) Very young children can be taught to respond each time they hear by dropping a block in a bucket, pointing to their ear, or raising their hand. These methods are called Conditioned Play. Instructions on how to train children to complete a detection task using a Conditioned Play response are below.
Young Children (Discrimination and Identification Task) You can help young children respond using a higher-level discrimination or identification response with the use of toys. It is easy to find toys to represent each of the Ling Six Sounds. For example, an airplane for the “ahh” sound and a snake for the “sss” sound. Instructions for how to train children to complete a discrimination or identification task are below.
Older Children (Identification Task) Older children can respond by pointing to a picture card that represents each sound or by simply repeating what was heard.
2) Aided audiogram – The free field audiometry procedure is carried out in aided condition and the response is plotted on an audiogram. The test should be carried out with 250 Hz to 4KHz. Testing of 8KHz is not important as most hearing aids do not provide amplification in that range. In very young children and infant aided behavioral response may be noted as they cannot be conditioned. The aided performance can then be compared to unaided response to see the amount of benefit. Moreover the aided assessment should be carried out at a regular interval and compared with the baseline measure. Any discrepancy should indicate problem with hearing aid or hearing.
3) Speech perception Tests – Many tests use speech material like nonsense syllables, words, sentences to assess the aided performance. The test is again carried out in a free field condition and the speech can be presented live through the audiometer, which the individual can hear via loudspeakers kept at a distance, in aided condition. The speech is presented at around 40 dBHL. Recorded material can also be used. For young children with limited vocabulary, picture identification tests can be used.
4) Questionnaires – various standardized questionnaires are used to get information about the benefit of the hearing aid. These questions are constructed for assessing the improvement in auditory/listening skills, communication skills, social life and quality of life. For very young children parental interviews are conducted to get information.
1.2 Ear moulds: Types, Importance, Care & maintenance
Earmolds are a component of behind the ear hearing aids. They are custom made to fit your ear exactly. Some fit in the bowl of your ear (the concha) and some fit in the canal.
Ears come in all shapes and sizes. Just take a look at any group of 10 people and you will see no set of ears are the same. Even your right and left ear can be shaped differently. That’s why behind-the-ear hearing aids require an earmold that is made to fit each person’s ear exactly.
If an earmold doesn’t fit properly, sound escapes the ear canal. The escaped sound is detected, picked up by the microphone, amplified and returned to the canal where it escapes again. With each iteration, the volume increases until you have a screeching or whining sound referred to as feedback. Feedback is a sign that your earmold doesn’t fit properly or isn’t inserted properly.
Earmolds versus domes
The parts of a hearing aid that fit inside the ear come in two basic styles: earmold or dome style. Earmolds are made of either plastic or silicone and custom-fit so that they sit snugly and precisely within the ear canal. They generally have small vents in them to let air through.
Dome styles, which look like small cones, are not customized to a person's individual ear shape. These are stocked in standard sizes and you are given the size that fits best in your ear canal. They generally have large openings to let in lots of natural sound and ventilation.
Depending on the type and degree of hearing loss, and the anatomy of the ear, the earmold can be canal size (small), half-shell size (medium) or full-shell size (large). The kind of earmold you wear also depends on your personal preference, the shape and texture of your ear, and your specific hearing aid.
An earmould is a piece of plastic that is molded to fit the shape of your ear. There are several parts to an earmould.
· A hole is drilled in the mold that will pave the way to your ear canal.
· A vent can also be made in the mold to improve sound quality. While vents can be a huge help with sound quality, they can also contribute to avoiding “occlusion” problems, which can make the sound of your own voice seem hollow or booming. Your hearing care professional may need to try a few different earmould set-ups before finding the one that is best for you.
· Tubing is mounted on the hook of your hearing aid to help direct sound from the hearing aid to your inner ear. Tubing is usually clear and almost invisible, but some people like to decorate their tubing or use fun colors
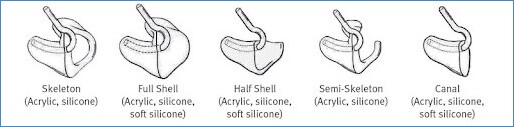
Two types of earmoulds can be made:
· Hard earmoulds: These are made with photoplastic material that cures with exposure to ultraviolet light. It is easy to keep clean and can be adjusted
· Soft earmoulds: These are made with silicone and are shaped according to the form of your ear. They are great for active children, and are mostly used for severe degrees of hearing loss.
The final product is shaped to have the desired acoustic properties and to conform with your hearing loss, hearing aid type, and the dimensions of your ear.
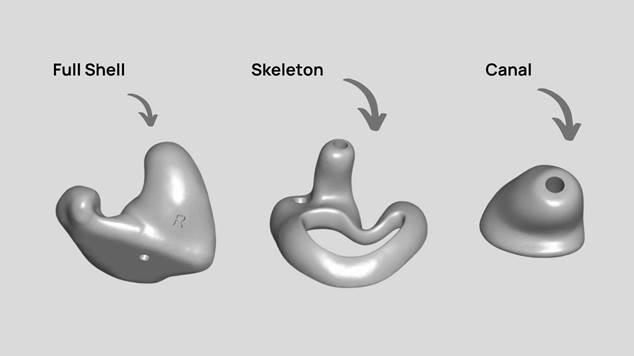
Full shell earmolds fill the entire concha of the ear. They are used for moderate to severe hearing loss because they provide maximum sound retention. Originally, these earmolds were made in “flesh” colored tones to make them less conspicuous. Today, they are made in a variety of colors to satisfy a wide range of tastes and styles.
Half-shell earmolds look like a full shell that has been cut in half on a horizontal plane. It is less visible than a full shell earmold but has many of the same benefits.
A skeleton earmold or semi-skeleton earmold is like the full shell, but a hole is cut out to make a ring around the bowl of the ear. The semi-skeleton earmold is easier to insert for people with dexterity issues.
Canal earmolds fit inside the ear canal and are made to be inconspicuous. They are made from an impression of the ear canal. These earmolds only work well for people with a fairly long ear canal. They are vented and tubed in the same manner as a full shell earmold.
Using your earmould
To insert your earmould, turn off your hearing aid or turn the volume down. The broad curve of the earmould should be towards the back of your head, and the elbow of the earmould should point upwards.
· Insert the earmould into your ear from behind at a slanting angle. It may be helpful to gently pull your outer ear backwards and upwards so that the ear canal widens and slightly straightens. Earmoulds slip easily into place in some people’s ears, while in others they must be gently “rocked” into place.
· When removing the earmould from the ear, turn off the hearing aid or turn the volume down. Then gently pull the earmould out of the ear.
Cleaning your earmould
It’s important to clean your earmould once or twice a week.
Follow these directions to clean your earmould:
· Carefully ease the tube, which is connected to the earmould, from the hearing aid hook.
· Rinse the earmould and tube in lukewarm running water.
· Put the earmould and tube in a bowl of mild soapy water or in an effervescent solution similar to that used for cleaning dentures. Let it soak for at least 10 minutes so that any earwax or dirt is loosened.
· Dry the earmould with a soft cloth.
· Let the earmould dry overnight on absorbent cloth or paper, with the sound outlet end of the earmould pointing down, so any remaining moisture can drain out.
· Attach the tube and earmould to the hearing aid.
IMPORTANT: Never put cotton buds, toothpicks, pipe cleaners or similar pointed objects into the earmould.
1.3 Classroom amplification devices: Individual, Speech Trainer & group, Hard wire, loop induction, infra-red & FM systems, their importance in educational management
In classrooms, where the area is large, the hearing impaired individual may face difficulties to hear speech of teacher and peers due to distance and effect of other factors such as noise and reverberation. In such situations hearing aids alone may not be useful; some additional assistive devices may be helpful. These devices can be useful for one individual at a time or can be used in a group of individuals.
INDIVIDUAL DEVICES
Speech Trainer: This device comes with a microphone for the speaker, the amplifier and headphones to be worn by the hearing impaired individual. The use of speech trainers have reduced in recent times, though many old schools still use these systems. The speech trainer comes with certain controls, where the output of the signal can be altered. The headset also comes equipped with a microphone, so that the user can hear own voice. This is also used during speech therapy sessions. Usually it is worn separately without the hearing aids.

Advantages
· The teacher’/trainer’s speech reaches the individual’s ear easily and is less affected by the noise and reverberation in the room. As the signal is going mostly in the ear canal, hearing becomes much easier.
· Usually these trainers come with high output capacity, so can be used for severe to profound hearing losses.
Limitations
· Since it’s a wired system, the mobility of the student and teacher is affected.
· Cannot be used in groups.
· Useful only for one to one teaching.
Personal neck loop system- The speech of teacher is picked up by a microphone worn by the teacher and sent to a loop worn by the student whose hearing aid is at telecoil position. The signal in the loop is picked up by the hearing aid and amplified.

FM System- These based on FM technology. These are typically used in schools. The teacher wears a microphone that is either clipped on to their collar or as a headset. This is connected to a transmitter, which sends out FM signals to the receiver unit worn by the student. It can also be carried around in the pocket everywhere. It helps reduce the background noise and improves speech clarity even at a distance. It can be used by a hearing impaired student in a normal classroom. It can be used as a individual or group device.
Personal amplified system
Personal amplifiers are useful in places in which the above systems are unavailable or when watching TV, being outdoors, or traveling in a car. About the size of a cell phone, these devices increase sound levels and reduce background noise for a listener. Some have directional microphones that can be angled toward a speaker or other source of sound. As with other ALDs, the amplified sound can be picked up by a receiver that the listener is wearing, either as a headset or as earbuds.
- A portable device that transmits sound via a microphone and transmitter to headphones, an earphone or a neck loop.
- Useful for one-on-one conversations or TV listening.
- Can be used indoors or outdoors.
GROUP CLASSROOM AMPLIFICATION DEVICES
Hardwired Assistive Listening Devices
Hardwired ALDs use an actual cord or wire to transmit the sound, thereby tethering the listener to the sound source. A hardwired ALD is typically lower in cost, easy to use, and is very portable. It is excellent for situations where the listener-to-speaker distance is not too great, such as in an automobile, restaurant or for TV viewing. It is also excellent as a temporary form of amplification such as may be needed in a doctor's office, hospital or nursing home. A disadvantage of the device is restricted mobility and limited seating arrangements which are dictated by the length of the cord. This limits the usefulness of a hardwired ALD in larger communication situations such as in a classroom, meeting or tour group.
There are five general types of assistive listening devices: audio induction (also called a hearing) loop, FM system, infrared system, personal amplified system and Bluetooth systems. The right device for you can depend on your hearing loss and where you need communication access.
Advantages
- Good for one-to-one communication, TV, car, restaurant or small groups
- Good for providing temporary amplification (i.e. hospital, nursing home)
- Good portability—battery operated
- Lower cost
Disadvantages
- Location and positioning of wires
- Limited seating options
- Cord length restricts application to small groups
Audio induction or hearing loop
Hearing loop (or induction loop) systems use electromagnetic energy to transmit sound. A hearing loop system involves four parts:
- A sound source, such as a public address system, microphone, or home TV or telephone
- An amplifier
- A thin loop of wire that encircles a room or branches out beneath carpeting
- A receiver worn in the ears or as a headset
Amplified sound travels through the loop and creates an electromagnetic field that is picked up directly by a hearing loop receiver or a telecoil (see sidebar), a miniature wireless receiver that is built into many hearing aids and cochlear implants. To pick up the signal, a listener must be wearing the receiver and be within or near the loop. Because the sound is picked up directly by the receiver, the sound is much clearer, without as much of the competing background noise associated with many listening environments. Some loop systems are portable, making it possible for people with hearing loss to improve their listening environments, as needed, as they proceed with their daily activities. A hearing loop can be connected to a public address system, a television, or any other audio source. For those who don’t have hearing aids with embedded telecoils, portable loop receivers are also available.
Advantages
- Cost benefit for users of telecoil equipped hearing aids
- Wire-free reception—freedom to move around within a specified area
- Good for TV viewing, meetings, one-to-one and groups
Disadvantages
- Seating restricted to looped area
- More involved installation limits portability and versatility
- Variability of signal strength within the looped area
FM system
FM systems use radio signals to transmit amplified sounds. They are often used in classrooms, where the instructor wears a small microphone connected to a transmitter and the student wears the receiver, which is tuned to a specific frequency, or channel. People who have a telecoil inside their hearing aid or cochlear implant may also wear a wire around the neck (called a neckloop) or behind their aid or implant (called a silhouette inductor) to convert the signal into magnetic signals that can be picked up directly by the telecoil. FM systems can transmit signals up to 300 feet and are able to be used in many public places. However, because radio signals are able to penetrate walls, listeners in one room may need to listen to a different channel than those in another room to avoid receiving mixed signals. Personal FM systems operate in the same way as larger scale systems and can be used to help people with hearing loss to follow one-on-one conversations.
- Transmits sound wirelessly via radio waves.
- The speaker wears a compact transmitter and microphone and the listener wears a portable receiver.
- The receiver may have a headphone, neckloop or other accessories.
- Commonly used for group meetings, church settings, conferences and classes. It may be used both indoors and outdoors.
Advantages
- Good flexibility and versatility for all listening situations
- FM signal is not obstructed by barriers, may be used outside
- Good portability—battery operated
- Wire-free reception with no seating restrictions
Disadvantages
- Potential for outside radio interferences
- Privacy if FM signal is received by other FM receivers
- High initial purchase price
- Transmitter and receiver must operate on the same FM frequency
Infrared system
Infrared systems use infrared light to transmit sound. A transmitter converts sound into a light signal and beams it to a receiver that is worn by a listener. The receiver decodes the infrared signal back to sound. As with FM systems, people whose hearing aids or cochlear implants have a telecoil may also wear a neckloop or silhouette inductor to convert the infrared signal into a magnetic signal, which can be picked up through their telecoil. Unlike induction loop or FM systems, the infrared signal cannot pass through walls, making it particularly useful in courtrooms, where confidential information is often discussed, and in buildings where competing signals can be a problem, such as classrooms or movie theaters. However, infrared systems cannot be used in environments with too many competing light sources, such as outdoors or in strongly lit rooms.
- Transmits sound wirelessly via invisible light beams.
- The receiver must be in direct line of sight of the light beam from the transmitter.
- Commonly used in churches, theaters and auditoriums. It can only be used indoors; sunlight may interfere with transmission.
- There are infrared devices made just for home television listening. The transmitter is placed on the TV and plugs into an electrical outlet. The user wears a battery-powered headset (receiver) with volume control. The TV volume can then be set at a comfortable level for other listeners.
Advantages
- High sound fidelity for music and speech—excellent for TV listening
- Infrared receivers are universal—will work with any IR transmitter
- Isolation of signal to the room—important if privacy is an issue
- Freedom from interference from outside transmitting sources
- Wire-free reception with no seating restrictions
Disadvantages
- AC-powered transmitter limits portability and versatility
- IR can only be used indoors
- IR signal is obstructed by barriers—requires line-of-sight reception
Bluetooth system
- Transmits sound via Wi-Fi.
- Works directly with hearing aids that have Bluetooth.
- Individuals with hearing loss who do not use hearing aids can use a smartphone or tablet with earphones to connect to the wirelessly transmitted sound.
1.4 Cochlear Implant, middle ear implant, BAHA & Auditory Brainstem implant: Candidacy, components, functioning & importance with special reference to ADIP 2014 scheme
Cochlear Implant
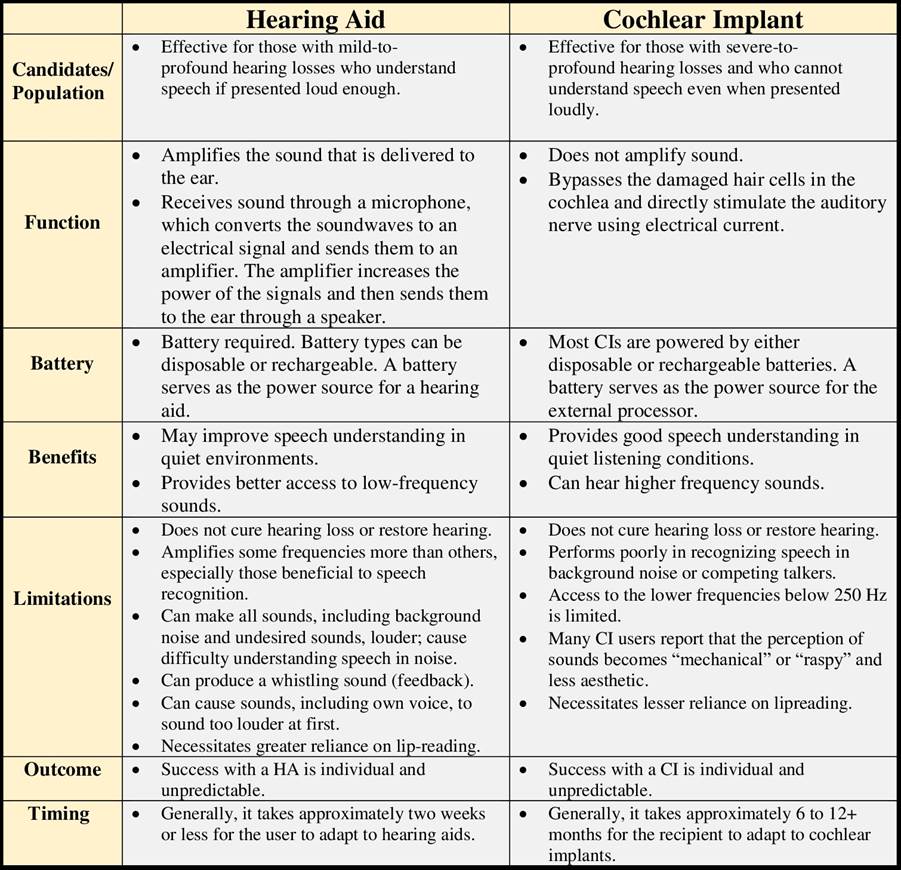
A cochlear implant is an electronic device that improves hearing. It can be an option for people who have severe hearing loss from inner-ear damage who are not able to hear well with hearing aids.
Unlike hearing aids, which amplify sound, a cochlear implant bypasses damaged portions of the ear to deliver sound signals to the hearing (auditory) nerve.
CANDIDACY
1. Hearing impaired individuals with severe to profound hearing loss.
2. Individuals who do not benefit from hearing aids or get limited benefits.
3. Individuals whose aided performance on speech perception tests is less than 50%.
4. No benefit from hearing aid, 3 months post fitting with hearing aids.
5. No other psychological deficits 6. No problems/disorders in higher processing centres.
7. Intact auditory nerve
These implants usually consist of 2 main components:
- The externally worn microphone, sound processor and transmitter system.
- The implanted receiver and electrode system, which contains the electronic circuits that receive signals from the external system and send electrical currents to the inner ear.
Currently made devices have a magnet that holds the external system in place next to the implanted internal system. The external system may be worn entirely behind the ear or its parts may be worn in a pocket, belt pouch, or harness.
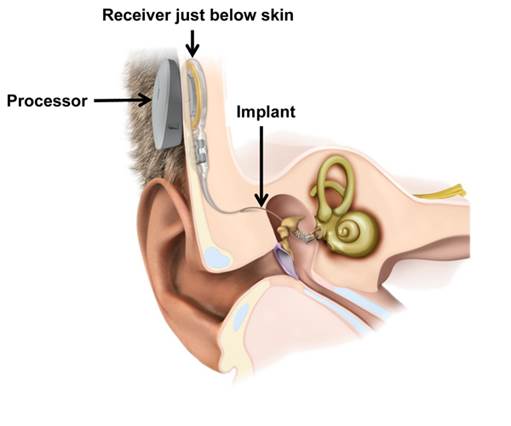
Cochlear implants use a sound processor that fits behind the ear. The processor captures sound signals and sends them to a receiver implanted under the skin behind the ear. The receiver sends the signals to electrodes implanted in the snail-shaped inner ear (cochlea).
The signals stimulate the auditory nerve, which then directs the signals to the brain. The brain interprets those signals as sounds, though these sounds won't be just like natural hearing.
It takes time and training to learn to interpret the signals received from a cochlear implant. Within 3 to 6 months of use, most people with cochlear implants make considerable gains in understanding speech.
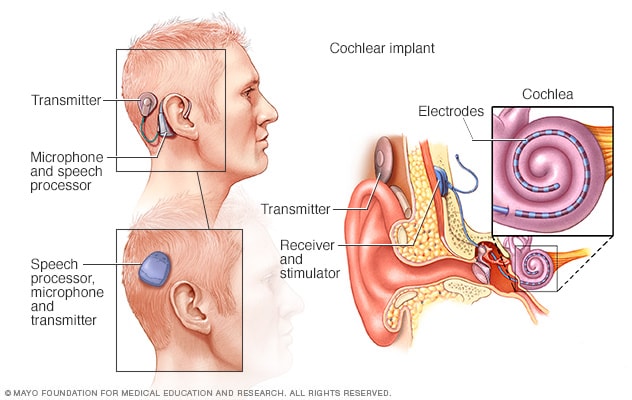
How cochlear implants work
A cochlear implant uses a sound processor that's worn behind the ear. A transmitter sends sound signals to a receiver and stimulator implanted under the skin. They stimulate the auditory nerve with electrodes that have been threaded into the cochlea. Some types of cochlear implants have one outside unit that has a speech processor, microphone and transmitter combined (lower left). Others have these as separate outside parts (upper left and on right).
Middle ear implant
Middle ear implants are suitable for those with a mild-moderate mixed or conductive hearing loss or a sensorineural hearing loss.
A middle ear implant is a more recent hearing implant, offering an alternative to conventional hearing aids. It may be considered for those who suffer with earmould allergies, skin problems in their ears, outer ear infections, narrow, collapsed or closed ear canals, or malformed ears.
It can also provide (for mixed or conductive hearing losses) an alternative to a bone anchored hearing aid for those with any of the above ear problems who also have healing issues, dexterity problems, or those who might find difficulty in keeping a bone anchored hearing aid clean.
A middle ear implant consists of an internal and an external part.
External part
The external component of the middle ear implant is the sound processor / audio processor which contains the battery, the microphone and the digital signal processing.
The sound processor / audio processor converts sounds into electrical signals that are transferred to the implant. The sound processor / audio processor is worn on the head and can be discreetly covered by the wearer’s hair. The sound processor / audio processor is held in place over the implant by a magnet in the implanted part.
Internal part
The internal component of a middle ear implant is surgically placed under the skin towards the back of the head. One part of the internal component is the Floating Mass Transducer (also called FMT), which is attached to a vibratory structure in the middle ear. The FMT vibrates specifically to each patient’s hearing needs, causing the structures of the ear to vibrate. These vibrations can be amplified and adjusted to compensate for different types and degrees of hearing loss. The FMT is the central component of a middle ear implant and is smaller than a grain of rice.
A middle ear implant works like this:
- Sounds are picked up by the sound processor / audio processor's microphone.
- The sound processor / audio processor converts environmental sounds into a digital signal.
- The digital signal is transmitted across the skin to the implant.
- The implant sends the signal via the conductor link to the Floating Mass Transducer (FMT) in the middle ear.
- The Floating Mass Transducer (FMT) converts the signal into vibrations that directly drive the middle ear structure.
- The vibrations conduct sound to the inner ear and to the brain.
CANDIDACY
· Individuals with mild to severe sensorineural hearing loss (the internal part will be different than in case of conductive or mixed hearing loss)
· Individuals with conductive and mixed hearing losses.
· Individuals who cannot tolerate foreign bodies in the ear canal for medical reasons, e.g., chronic ear canal inflammations or ear canal eczemas.
· Individuals who require a free ear canal for personal or professional reasons, e.g., musicians, singers or physicians.
|
There are two types of MEIs – piezoelectric and electromagnetic. The piezoelectric approach, pioneered by Drs. Suzuki and Yanagihara, uses a piezoelectric crystal, which has an interesting property– applied electric charge can cause the crystal to bend and a bent crystal generates electric charge. The crystal can function as a microphone, generating electric charge in response to incoming sound waves which bend the crystal, and as a driver (when attached to the middle ear bones), moving in response to electric charge from the microphone. This causes the middle ear bones to vibrate and transduce sound to the inner ear. The electromagnetic approach uses an external microphone and sends the signal through an inductive coil that creates a magnetic field. The implanted receiving coil picks up this signal and connects to a transducer attached to one of the three bones and vibrates in synchrony with the magnetic field. Sound is then transduced to the inner ear. One advantage of the piezoelectric approach is that the components of the implant are physically small, allowing a fully-implantable system. Its design is also simple. In contrast, the electromagnetic approach uses bulkier components and are only partially implantable. Its design can also be complex. However, compared to the piezoelectric approach, the electromagnetic approach can provide significantly more gain and output and can be used for patients with severe hearing loss. The piezoelectric approach is limited to patients with mild to moderately severe hearing loss due to its limited output gain. |
Bone-anchored Auditory Implant
A bone-anchored auditory implant is a surgically implanted device for the ear. The implant can help provide hearing for people with:
- Conductive hearing loss or mixed hearing loss (when sound is not traveling through the ear well).
- Single-sided deafness (one ear is typically functioning, the other has little to no hearing).
There are several types of bone-anchored auditory implants. They usually consist of a small implant placed behind the ear and a sound processor attached to the implant. Together, they send sound as a vibration to the inner ear and hearing nerve.
In some implants, the sound processor attaches to a small titanium post that comes through the skin. In others, a magnet holds the sound processor in place and the implant is not visible.
For children younger than 5 years old, or for those who may not prefer a surgical option, some sound processors can be held in place with an elastic band or strong adhesive sticker.
Unlike hearing aids, bone-anchored hearing systems are surgically implanted devices. They treat hearing loss through bone conduction of sound vibrations to the inner ear—this is in contrast to regular hearing aids, which amplify acoustic sounds that enter the ear canal.
For this reason, bone-anchored systems are considered specialty devices for people who have outer or middle ear problems, but at least one functioning inner ear (cochlea).
Bone-anchored hearing systems (BAHS), also known as bone-anchored auditory implants or bone-anchored hearing aids (BAHA), are not to be confused with cochlear implants. While they are also a type of surgically implanted device for hearing loss, the patient indications are different. In other words, they treat different hearing problems.
COMPONENTS: BAHA has 3 components. They are :
1. Titanium screw that becomes integrated with the skull bone behind the ear.
2. Titanium abutment is fitted to the titanium screw which is already integrated to the skull bone.
3. Ear level sound vibrator.

Functioning of BAHA
Bone-anchored hearing devices have two parts: a titanium bone implant and an external sound processor. The external microphone and sound processor of the bone-anchored device picks up sounds and converts them into vibrations to the embedded implant. In turn, the implant vibrates the surrounding bone, which sets up sound waves in the inner ear that stimulate the hair cells and result in the firing of the auditory nerve.
A bone conduction hearing device offers amplification without an ear mould in the ear. This makes them more comfortable if you experience discomfort or infections in your ear. Some people also report that they have a more natural sound than conventional hearing aids for the same reason. They do not restore your hearing to normal, but can make managing in everyday situations easier.
A bone conduction hearing device is compatible with hearing loop (telecoil) systems. You can select to pick up sound through the microphone, through the loop, or through a combination of both microphone and loop. This means you can take advantage of assistive listening devices, neckloops or switching to ‘T’ in places displaying the ‘T’ symbol. The bone conduction hearing device processor may have the telecoil feature integrated within it. Otherwise a telecoil accessory can be plugged into the processor when needed.
CANDIDACY
1. Individuals with bilateral canal atresia is an indication for the use of BAHA. This is because canal atresia prevents insertion of an air conduction aid.
2. Individuals with chronic ear infections when insertion of ear moulds is a problem.
3. Individuals with unilateral hearing loss who cannot benefit from use of regular hearing aids. (sensory neural, but good bone conduction hearing)
Importance of BAHA
1. It is a device of choice for individuals who cannot be fitted with conventional hearing aids. This can be due to a variety of factors, such absence of external ear, middle ear infections with active ear discharge.
2. It is also useful for individuals with unilateral sensorineural hearing loss (bc upto 55dBHL)s
Auditory Brainstem implant
An auditory brainstem implant provides hearing to people with hearing loss who can't benefit from a hearing aid or cochlear implant. This is most commonly due to a missing or very small hearing nerve or severely abnormal inner ear (cochlea). The auditory brainstem implant directly stimulates the hearing pathways in the brainstem, bypassing the inner ear and hearing nerve.
Auditory brainstem implant was originally developed for adults diagnosed with neurofibromatosis type 2 — a rare genetic condition that causes tumors to grow on nerves. The surgery is now considered for adults and children with other nerve and inner ear abnormalities.
This type of implant bypasses the cochlea and auditory nerve to directly stimulate auditory pathways of the brain. Patients that are not good candidates for a cochlear implant due to severely damaged or missing cochleas or auditory nerves may benefit from an auditory brainstem implant.
Components of ABI
The ABI bypasses parts of the ear that are absent or no longer work properly by sending signals directly to the brainstem.
1. A microphone on the sound processor, worn behind the ear, picks up sounds and converts them to digital information.
2. A receiver-stimulator, implanted under the skin, uses the digital information to provide electrical signals to an array of electrodes.
3. The electrode array provides electrical stimulation to neurons of the auditory brainstem.

Functioning of ABI

A surgical approach known as translabyrinthine (through the inner ear) or retrosigmoidal (behind the ear) will be used to gain access to the electrode placement site.
After the electrode is placed on the brainstem, the receiver-stimulator is anchored into the bony wall of the skull.
The electrode array will be tested to ensure activity and stimulation of auditory responses and to make sure the electrode is not stimulating other nerves.
Most patients spend two to four days in the hospital following surgery. They will have a follow-up visit one or two weeks afterward for evaluation of wound healing. Four to six weeks after surgery, the implant will be activated (turned on) and programmed to sound levels appropriate for the patient.
CANDIDACY
1. Individuals of atleast 15 years of age.
2. Individuals with damaged auditory nerve due to conditions like tumour of auditory nerve (NF2), where the auditory nerve(s) are irreversibly damaged
ADIP Scheme 2014
Scheme of Assistance to Disabled persons for Purchase/ Fitting of Adis/Appliances (ADIP Scheme) 2014
It has been the constant endeavor of the Government to provide the disabled persons with aids/appliance, at minimum costs, which are essential for their social, economic and vocational rehabilitation. Census, 2011 states that there are 2.68 crore Persons with Disabilities (PwDs) in the country. In addition, about 3% of the children below 14 years of age suffer from delayed development.
Many of them are mentally retarded and cerebral palsied and require aids/appliances to attain the capacity for self-care and independent living. With the application of modern technology, a number of aids have emerged which can reduce the effects of disabilities and enhance the economic potential of the disabled. However, a large number of disabled persons are from the low income groups and are deprived of the benefits of these appliances because of their inability to find funds to acquire them and consequently of dignified independent living.
In the light of the Government’s commitment for enabling and empowering disabled persons, it has been decided to continue and modify ADIP Scheme in such a way that it becomes more user-friendly and the needy are not deprived of necessary aids /appliances for want of means to acquire them together with a transparent mechanism for checks and balances.
Main Objective
The main objective of the Scheme is to assist the needy disabled persons in procuring durable, sophisticated and scientifically manufactured, modern, standard aids and appliances to promote physical, social, psychological rehabilitation of Persons with Disabilities by reducing the effects of disabilities and at the same time enhance their economic potential. Assistive devices are given to PwDs with an aim to improve their independent functioning, and to arrest the extent of disability and occurrence of secondary disability. The aids and appliances supplied under the Scheme must have due certification.
The Scheme will be implemented through the Implementing Agencies as following Agencies. The Agencies will be given financial assistance for purchase, fabrication and distribution of such standard aids and appliances that are in conformity with objectives of the Scheme. The Implementing Agencies will take care of/ make suitable arrangements for fitting and post-fitting care of the aids and appliances distributed under the Scheme.
The Implementing Agencies will give wide publicity of the distribution of such aid and appliances to PwDs. Further, before the camp they will inform the District Collector, BDO, a local public representative, State Government and the Department of Disability Affairs at least one week in advance about the date and the location of the camp. After the camps, they shall provide a list of beneficiaries and the details of aids and assistive devices with the cost incurred to the State Government and the Department of Disability Affairs. The list of beneficiaries shall be prominently displayed in the website of the Implementing Agency.
The Scheme shall also include essential medical/surgical correction and intervention, prior to fitment of aids and appliances, as per the following norms:
1. From Rs.500/- to Rs.1,000/- for hearing & speech impaired.
2. From Rs.1000/- to Rs.2,000/- for visually disabled.
3. From Rs.3000/- to Rs.5,000/- for orthopedically disabled
Eligibility of the Beneficiaries
1. An Indian citizen of any age.
2. Holds a 40% Disablement Certificate.
3. Has monthly income from all sources not exceeding Rs. 20,000/- per month.
4. In case of dependents, the income of parents/guardians should not exceed Rs. 20,000/- per month.
5. Who have not received assistance during the last 3 years for the same purpose from any source. However, for children below 12 years of age, this limit would be one year.
Candidacy for Cochlear Implant under ADIP Scheme
· Children with severe to profound sensorineural hearing loss in both ears and who do not receive any benefit with hearing aids.
· For pre-lingual or at birth hearing impairment, preferred age for CI is between 1 to 5 years
· If hearing loss is post lingual /acquired after 4-5 years of age, preferred age for CI is less than 12 years
· Child should not have any co-existing disabilities like cerebral palsy, cognitive impairment or other developmental disabilities.
· Child should have Disability Certificate prior to CI
· 100% subsidized cochlear implantation is available for children with family income upto 15,000/- per month and 50% subsidy is provided for children from families having a monthly income upto 20,000 and no subsidy is provided for income above that.
1.5 Comparison between individual hearing aids, group hearing aids & cochlear implant and their care & maintenance
Individual hearing aids are fitted to individuals with hearing loss (anywhere between mild to severe). There a variety of options possible in individual hearing aids. Individual hearing aid’s performance depends on the technology used. Digitally programmable ones are highly recommended for their better performance. In this category also there are plenty of options available commercially. The advantages of individual hearing aid is it can be used by the individual according to own requirements. The mobility is not restricted. The user can upgrade his/her hearing aid as and when required.
There are certain limitations, the cost of a new hearing aid has to be totally born by the individual totally (socially backwards can apply under ADIP scheme. These hearing aids undergo regular wear and tear, so they need to be changed at every 5 years (appx).Hearing aids are electronic devices, may need servicing and repair. The cost of service and repair again has to be born by the individual.
CARE AND MAINTENANCE
· It should be kept clean and free from moisture. - after every use, should be cleaned with a dry cloth and kept back.
· The battery should be removed, when not in use. Batteries to be changed regularly.
· Hearing aid should be removed during bath.
· It should be sent for regular servicing. 5. It should not be dropped from a height.
· It should not be exposed to excessive heat and strong electric/magnetic field.
· Hearing should be checked at a regular interval, hearing aid or settings should be changed in case of change in hearing thresholds.
· The overall life of a hearing aid is about 5-8 years. It should be changed at that interval.
· In case of any problem it should be taken to audiologist.
· In classrooms, teachers can keep a regular check on the functioning of hearing aids worn by the students. The switches, battery, and overall condition of the hearing aid to be checked regularly. Even the sound quality to be checked regularly.
Group Hearing aids
The onus of care and maintenance of the group hearing aids is usually on the institutional set up, where it is used. The hearing aids are set at a same level, so individual requirements are difficult to address. One to one communication training/teaching is difficult. Mobility of the students get restricted. It is less often used.
However the overall cost of the system and maintenance cost is more economical.
Both hearing aids and cochlear implants help people with hearing loss to communicate better. Hearing aids do not require surgery and are best suited for people with less severe hearing loss and fair speech understanding. Cochlear implants require surgery and are best suited for people with more severe hearing loss in one or both ears and poor speech understanding.