Unit 2: Technology for Management for Speech
2.1 Computer based training aids/equipment for management of speech (Dr. Speech; Vaghmi; Speech viewer)
2.2 Use of computer based speech equipment for management of voice in children with hearing impairment
2.3 Use of computer based speech equipment for management of suprasegmental features of speech in children with hearing impairment
2.4 Basic infrastructure required for using computer based speech training aids/equipment
2.5 Tele Speech Therapy
2.1 Computer based training aids/equipment for management of speech (Dr. Speech; Vaghmi; Speech viewer)
Unintelligible speech makes it difficult for an individual to fully function in a social setting and can be a social handicap. Difficulties in producing the different speech sounds and problems modifying the pronunciation may arise from the individual not hearing what is wrong because of reduced hearing or learning a language different from the mother tongue. Speech therapists and language teachers can help to correct the pronunciation, but the amount of help that they can provide is limited. Some children with speech deficits meet the therapist as little as 30 minutes a month.
Speech learning and speech training can be improved by the use of another modality than hearing. Due to the problems hearing the mispronunciation, it is important to show where and how the articulation is produced and how different speech sounds differ from each other. The most important parts of the learning process are feedback of the articulation and repeated practice, which is performed with the help of a therapist.
There is a wide consensus that computer-based speech training (CBST) systems are useful tools in speech training. However, they are not suitable for all the needed exercises and a major drawback is that they usually require help from educated personnel.
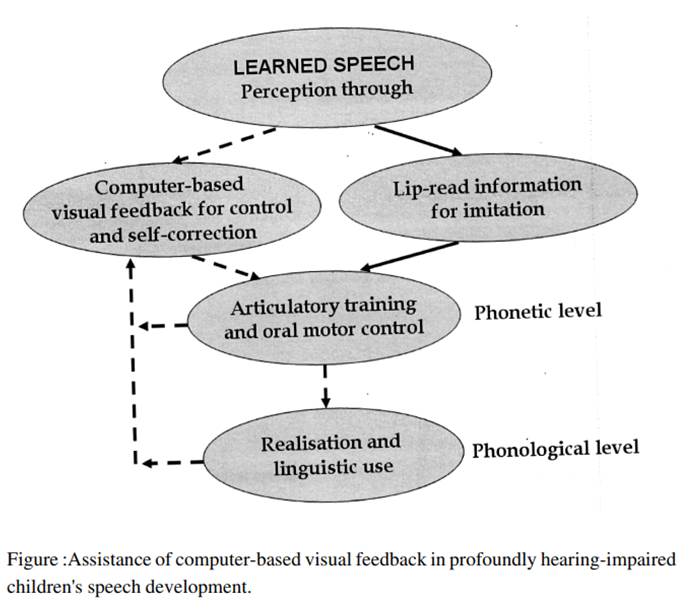
Computer-based speech training has capabilities of offering the children immediate and meaningful visual feedback and might make it easier for the teacher to instruct and explain what is wrong and what is correct and through motivational and frequent training establish an intelligible production. In most schools for deaf children in Sweden, computer-based visual speech training has become a standard and valuable complement to the regular speech-training activities.
Hard of hearing have vocal organs which are normal and hence can produce speech. This is especially so if they have some language ability. That is, if a child has acquired deafness after having exposed to hearing the language. Hence the dictum “deaf need not be dumb“. The reason that they may not be able to produce speech is because of the lack of auditory feedback, i.e., inability to hear what they have spoken and hence unable to correct what is spoken if it is incorrect.
· Picture-Word-Articulation test may be used for an evaluation of the pronunciation errors. Exercises may be given to correct the pronunciation errors.
· Their dependency on lip reading sometimes leads to mis-pronunciation of speech sounds. For example, ‘p’, ‘b’ and ‘m’. Nasal indicator may be used to make them aware of the production of nasals.
· Also, the hard of hearing often lack ‘breath support’. That is they are unable to speak for a long duration in a single breath and they have to take breaths often. Their breath support has to be improved.
· Further, a hard of hearing child tries to speak at a very loud voice or shrill voice since for the child itself they sound normal. In course of time this leads to voice abuse and possible damage of the vocal folds (the voice box). This can be prevented by a proper voice control.
· Some hard of hearing children speak with a mono-tone pitch or dull voice. They lack proper intonation and their voice will not be lively.
Dr. Speech
TigerDRS is a trusted, leading voice & speech therapy products and services platform designed for personal and professional use, private practices, hospitals, clinics, schools, etc. Founded in 1992, goal from the start was to help and improve those with speech, language, communication, brain disorders, etc. by offering products and services that focuses on individualized therapy. Tiger DRS. Inc, USA released Dr.Speech highly advanced clinical & educational tools for speech - language pathologist, voice teacher, laryngologist, deaf teacher and special educator.
Dr Speech is clinical software which provides valuable assistance during assessment and treatment of voice and speech disorders in children with hearing impairment. Demographic information, such as names, address, number of visits, types of disorders, progress reports, insurance claim, etc. is easy to display. When such clinical software is installed in a laptop computer, it provides clinicians with a "portable clinical voice laboratory" equipped with powerful clinical tools that easily can be carried from one treatment location to another. Today’s practitioners can benefit from the use of clinical software that has been adapted to the needs of clinicians.
Products
Vocal Assessment provides you with the ability to analyze and display both acoustic and EGG features of a sustained vowel. A wide range of parameters (jitter, shimmer, NNE, etc.) and graphic displays (spectrogram, F0, intensity, etc.) are offered. Used to guide diagnostic assessments for voice disorders by measuring hoarse, harsh, and breathy voice.
Key Features:
· Real-time dual-channel recording
· F0, jitter, shimmer, glottal noise, ratio
· Contact quotient, Contact index
· Spectrogram, spectrum
· Voice quality (hoarse, harsh, breathy)
· Vocal function (regularity, closure time)
· Built-in voice database
· Clinical progress tracking
· Video capture and e-mail compatible
Real Speech is a real-time biofeedback tool used in both clinical and educational environments. It’s used to guide diagnostic assessments for speech disorders by measuring respiration, phonation, and resonance.
AAC uses non-verbal communication training during the early-language stage. Provides 384 core words for rehabilitation training. The goal of this software is to help develop a reasonable and personalized treatment program that may be used for therapy at home.
My Words: Interventions for early speech disorders: provides comprehension and communication training for basic words, core nouns, core verbs, numerals, and adjectives.
Key Features:
· Introduces early vocabulary of Noun, Verb, Numeral, Adjective
· Provides colourful picture , script , IPA of each word
· Displays pitch contour
· Modulated speech pre - recorded output
· Activity based programs puzzle, skill bulider
· Communication board interfaced
Nasal View is a cost-effective software/hardware system designed for the data acquisition, clinical analysis and treatment of nasal resonance disorders. It’s a powerful clinical and teaching tool that provides highly versatile information for speech assessment and therapy features pertaining to resonance disorders.
Key Features:
· Real-time biofeedback
· Nasalance & dual oscillograms
· Nasalance statistics & histogram
· Power & LPC spectrum
· Vocal F0 & intensity
· Model-matching features
· Wide & narrow-band spectrogram
ScopeView is a real-time video and analysis system designed for voice professionals, otolaryngologists and throat patients with advanced tools. It can capture images via fiberoptic, rigid laryngoscope, microlaryngoscope, video camera or video recorder to help doctors store, analyze, process and print images of the throat.
Phonetogram is a real-time vocal ability assessment system that may be used as a powerful clinical and teaching tool to help analyze, document and report vocal ability in various applications. It displays the dynamic range of the human voice with both fundamental frequency (pitch) and intensity (loudness). This software is useful in identifying the limits of vocal function.
Key features:
· On-screen piano to play tone
· Power cursors for quick measures
· Comparison of multi- sessions
· Monitor the vocal progress
· Statistic report
Pitch Master provides diagnosis, evaluation, rehabilitation training and guidance for speech, language and prosody disorders by using real-time audiovisual feedback technology. Key functions include real-time feedback and training of vowels and consonants using lento, andante, and allegro (tempo), as well as real-time training of consonants using the accent method.
Speech Training software is a real-time dual-screen speech assessment and training system that helps analyze, document, teach, reinforce and report speech waveform in various applications. It’s a powerful clinical and teaching tool that provides highly versatile information for speech assessment and therapy features.
Key Features Speech training/Pitch master:
· Real-time capability
· Dual-screen display
· F0 and intensity display
· Spectrogram display
· Formant tracking display
· Speech waveform display
· Power and LPC spectrum
· Dynamic vowel tracking
· Quick statistic report
· ESL training
Speech and voice Therapy uses over 30 voice-activated interactive and entertaining games providing real-time reinforcement of changes in pitch, loudness, voiced and unvoiced phonation, voicing onset, maximum phonation time, sound and vowel tracking.
Key features:
· Biofeedback
· Interactive cartoon
· Over 70 video games
· Phonation Articulation
· Statistical report
· Clinical goal settings
Vagmi
Established
in the year 1989, Voice and Speech Systems, is one of
the renowned organization, engaged in providing Voice Speech Software
services to our valued clients across the nation. Our range of
services includes Voice Speech Software: Speech Games, Vaghmi-Pro Voice
Therapy, Vaghmi-Pro Articulation Therapy, VAGHMI Therapy Software, Vaghmi Voice
Therapy Software, Vaghmi Articulation Therapy Software, Vaghmi Disfluency
Therapy Software, Vaghmi Voice Diagnostics, Disfluency Diagnostics and Therapy
and Vaghmi-Pro Diagnostics. Apart from providing this service, we are also
offering active filter products of international quality
standard. We conduct Basic Research in the area of Speech Signal Processing,
which is enabling us enhancement of our Product in the area of Speech and
Hearing.
Therapy modules are easy to
use software tools that effortlessly convert P.C. into therapy equipment. No
programming skills are required to use these modules and even your child can be
his or her own therapist. These modules are visually appealing with exciting
graphics and re enforcement messages. Using Vagmi therapy modules, clinical
reports to great scientific accuracy can also be generated. The following are the
therapy modules:
· Voice Therapy
· Articulation Therapy
· Nasalence Therapy
· Disfluency Therapy
· Picture-Word Articulation Test
Vaghmi Articulation Therapy Software
Vaghmi Articulation Therapy is useful to
· Hard of hearing and Spastics.
· Normal persons with mis-articulation problems.
·
Stroke
patients.
What is Articulation Therapy?
Mis-articulation is a
common problem even amongst normals. Children often mis-pronounce fricatives
such as 's', 'sh' etc. 'Deaf needn't be dumb'.
They have normal control over articulation. Problem of hard of hearing is much
more complex. As they rely on lip-reading, they mis-articulate sounds 'b', 'p' and 'm'.
Voice (g,d,b) Vs Unvoice (k,t,p) distinction
is another major problem. Stroke patients have to undergo speech therapy to
regain speech. Listening to one's own tape-recorded voice or standing in-front
of a mirror is not an effective therapy technique.
Vaghmi_Pro Articulation Therapy is a sophisticated software tool that
converts a PC into a therapy equipment. What used to be monotonous and time
consuming has now become interesting, effective and time saving.
Vaghmi_Pro Articulation Therapy provides a visual feedback of
articulation process and displays the measured parameter in comparison with a
model. The articulation of the phoneme can be shown in a Script of a language
of user's choice such as English, Hindi, Kannada etc. It has many interesting
Games, Puzzles etc with powerful visuals. Stimulating tasks are to be achieved
during therapy. The performance is scored. Reinforcement messages appear. Goals
can be set in a graded manner.
Articulation Therapy Sub-Modules
Vowel Therapy: Production of vowel sound can be learnt using this
module. As the subject phonates a vowel, a display of First Vs Second formant
is shown as a dot which ideally must be inside a marked rectangle.
In another program the measured distinctive feature High-Low Vs
Front-Back is shown. The effect of moving the various articulators
such as tongue and jaw on the formant locations or distinctive features can be
visualized. Thus proper articulatory positions can be learnt.
Tongue is usually well hidden. But, by means of acoustic analysis, when the
subject phonates a vowel, the measured tongue shape is shown
against the tongue profile of a model.
Fricative Therapy:
This program can be used for cases with disability to produce and sustain
frication. Also, there are Fricative Therapy programs to teach s Vs sh distinction
and s Vs z distinction. In Sun-Rain sun shine
is shown when a vowel is produced and rain fall is shown when a fricative is
produced.
See and Speak
See Vocal Tract Shape: This displays the mid-sagittal vocal tract shape
(profile) indicating the ideal articulatory positions for sustained sounds and
CV syllables.
Lip Reading: To facilitate the learning of lip reading, front view of the face is
shown.
See Speech Signal: Speech signal corresponding to various sustained sounds
can be shown in split screen format. This acts as an oscilloscope.
See Speech Spectrum: Speech spectrum is shown. Spectra of subject and model
can be compared for the same sound or specra for different sounds, such as 's'
and 'sh', can be compared.
Vaghmi Voice Therapy Software
What is Voice Therapy?
Voice therapy involves certain exercises related to the use of voice just like physio therapy. The vocal exercises to be practiced with respect to one or more attributes are prescribed by a professional. Usually each sessions lasts for about 20 minutes and with about 2-3 sessions per week and the sessions may last over several months.
What are voice attributes?
Voice
quality is determined by Respiratory, Laryngeal and Articulation (Nasality)
controls. Phonation duration; pitch or fundamental frequency F0; intensity etc.
are some of the voice attributes which can be measured and which are related to
the resipratory, laryngeal and articulatory controls. The therapsi sets the
goal to be achieved with respect to one or more voice attributes.
Vaghmi Voice Therapy Software
Vaghmi-computerized voice therapy software is a sophisticated tool that converts a PC into a therapy equipment. It has interesting games, puzzles, stimulating tasks to motivate the user to practice.
It measures the voice attribute being practiced by the client. The software compares it against the goal to be achieved and gives a feedback.
Who needs voice therapy?
People generally believe that ''voice'' is something that one is born-with. But, voice quality can be changed by therapy to make it less abusing to vocal folds and more endearing to the listeners.
Even persons with ''normal voice'' may be improperly using voice production
mechanism by habit leading to long term problems.
Professionals who use voice extensively such as teachers, lawyers, singers etc
may be unaware of the voice dimensions. He/she has to be doubly sure that the
voice production mechanism is being used optimally to avoid long term
complications.
A singer has to use the optimum pitch. A singer has to make sure that he/she is
hitting the notes correctly. Therapy programs helps them.
''Voice Quality'' being used may be such that one gets easily tired even after
a brief interval of speaking or singing.
''Voice Quality'' being used may be such that the listener has to strain to
understand one''s speech.
A person who speaks too loud or too soft or is unable to control voice properly
need to be aware of voice therapy.
A normal male person''s voice may sound feminine (puber-phonia). Therapy helps
in such cases. A person''s voice may be highly nasal. Therapy may help.
A normal child may require voice and speech therapy due to improper learning.
A child with hearing impairment or a cochlear implant lacks good auditory
feedback. They can have normal voice. A spastic child lacks muscular
coordination. Parents of such children need to be aware of voice and speech
therapy.
Vaghmi Disfluency Therapy Software
Disfluency Diagnostics and Therapy is provided by the speech pathologists to diagnose per centage disfluency and to the persons with stuttering problem.
Disfluency diagnostics
The stutter's speech is recorded and the signal waveform is displayed, in disfluency diagnostics. After which the pathologist marks the various blocks manually. The program gives in a tabular form and given duration of various types of blocks. It is also capable of measuring the per centage disfluency.
Disfluency therapy
The speech pathologists use various techniques to improve a person’s speech and help him get rid of the stuttering problem, which might be occurring due to various reasons
Modules
Daf: like echo, delayed auditory feedback continuously plays back the subject's speech after a set delay. The delay can be between 50 to 500 msec. Headphone is used to play the delayed speech to the subject. This process goes-on till stopped. The optimum delay depends on the subject and is arrived at by trail and error. The subject is asked to read a passage. To facilitate this, a text file can be loaded for the user to read instead of reading from a book.
Prolongation: to normalize the rate of speech, the subject has to read passages at a slow rate. For this purpose pre-recorded normal speech signal can be stretched by desired factor and played as a reference. Subject can imitate the reference.
Slide text: pre-written text in a file can be loaded. The text is then presented at a controlled rate either as sliding text or a few words at a time. The subject has to read the text keeping in pace with the rate of display. This process improves the control of rate of speech.
Metronome: represents a rhythmic rate of beats. The rate can be set. The beats are presented in visual and/ or auditory mode. This acts as a reference. The subject has to read the text keeping in pace with the rate of beats. This is to make a rhythmic speech. The rate of beats starts with a slow rhythm and then becomes normal..
Noise: white random noise is generated and is played over the headphones to suppress the auditory feedback. The subject has to read a passage while the noise is being fed to the ears.
Vagmi Picture-Word-Articulation (PWA)
Module can be used
(a) As a Phonic drill to (test) evaluate the pronunciation of speech sounds for the hard of hearing as well as children with normal hearing and identify the sounds whose pronunciation have to be corrected
(b) For stroke patients in helping memory recall
(c) To learn a secondary language at word level
This module is currently available in English, Kannada, Telugu, Hindi, Oriya, Arabic, and is easily programmable by an experienced user to any desired language. Also, the existing test can be modified by adding various different pictures and sound clues. A parent supervisor or a therapist or a special teacher accompanying the client grades the pronunciation as ‘poor’, ‘just ok’, ‘fair’; ‘average’, ‘good’, etc. A corresponding reinforcement is given. The score achieved is saved. Pictures and words for all the speech sounds of a language may be tested in the picture-word-articulation test. Based on the overall performance, the next step to be followed can be decided. For example, after the test, if it is observed that the client is unable to pronounce the ‘s’ sound properly, then the test can focus only on the ‘s’ sounds.
Speech viewer III
SpeechViewer III is a powerful speech and language tool that transforms spoken words and sounds into imaginative graphics. SpeechViewer III increases the effectiveness of speech therapy and speech modification for people who have speech, language or hearing impairments.
You can select from over a dozen SpeechViewer exercises. Each exercise responds to your voice input with immediate, clear and meaningful feedback that helps you “see how to speak.” In addition, SpeechViewer III provides animated rewards that reinforce successful responses.
The software incorporates the latest SVGA graphics, a revised menu bar format for access to clinical exercises, point-and-click capability, pull-down menus, and enhanced phoneme (a word, phrase, or sound) model creation. The program’s sophisticated clinical management functions automatically collect pertinent data that allow therapists to easily document progress and see and hear results.
SpeechViewer III is designed to help people of all ages who have a variety of disabilities, such as speech or language impairments, cerebral palsy, developmental delay, traumatic brain injury, and speech disorders resulting from a stroke. It is ideal for professional speech language pathologists, special education teachers, teachers of the deaf, English as a second language instructors, professionals working with accent reduction and others.
SpeechViewer III augments traditional procedures for treating speech, language, and hearing disorders, and dialects associated with English as a second language. Professionals can gain control over speech attributes, such as voice, pitch, loudness, sustained phoneme production accuracy, and speech timing.
New clinical and client management features include:
- Sound -- for interactive displays of a client's loudness, pitch, and voice
The exercises vary in complexity and in the sound features displayed:
- Sound presence
- Loudness range
- Pitch range
- Pitch control
- Voice presence
- Voice onset
- Voice timing
- Phonology -- for activities using a phoneme model created by the client and clinician
- Phoneme accuracy
- Two-Phoneme contrast
- Four-Phoneme contrast
- Multiphoneme contrast
- Patterns -- for activities demonstrating the patterns of continuous speech production
- Pitch and loudness patterning
- Waveform
- Spectrogram
- Spectra patterning
The Clinical Management Functions include:
- Save speech samples in a client’s progress report or for use in lessons at a later time.
- Modify and save screen designs to aid in individualizing treatment programs
- Save individual client settings (with passwords for privacy and maintenance of integrity of data)
- Display and save statistics on client performance
- Write clinical notes and print reports that show clinical objectives and client progress with exercises
- Print copies of SpeechViewer III screens to record progress
- Copy, move and delete client data
SpeechViewer III also supports a full range of clinical activities -- from creating awareness of speech elements to building skills in using those elements. Selections from the menu bar help to determine which exercises work with different speech parameters. All exercises provide auditory playback synchronized with the graphic display of speech patterns. The audio can be played back at normal or slow speeds. SpeechViewer motivates clients through the use of graphics and game-like strategies. Each exercise has a variety of graphic designs to keep the therapy sessions interesting and fun, for children and adults.
Clinicians can use SpeechViewer to:
- Save speech samples to record progress or recall as lessons
- Create and save screen designs (in some exercises) to individualize treatment programs
- Display and save statistics on client performance
- Print SpeechViewer III screens for record keeping
- Copy, move, and erase speech samples, screen designs, phoneme models, notes, and statistics
The Exercises Menu
· Each exercise is very clearly listed and described in the User Guide and in the Online Help system. The Purpose, Starting and use of the Settings sections are easy to understand and follow, even for a lay person! The 34-page tutorial is a comprehensive guide to using SPV3 more effectively and provides excellent background information as to its usefulness and application.
· When you choose a client ID, or click on Start, you are presented with a menu with 13 items. These include:
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
· On the Menu Bar you see four groups. These each suggest exercises that you might consider for each speech parameter. The groups are Pitch, Prosody, Voicing and Phonology. Each of the exercises has a sub menu (e.g. Sound Presence has Alien, Dog, Flamingo and Kaleidoscope). Some will suit younger clients, whilst others will appeal to older users. At the base of the screen appears a Status Bar. It indicates such things as the conditions that have been set, who is speaking (the clinician or the client), the integrity and status of the statistics, whether the threshold is too loud and shows the microphone status (on or off).
The Settings Menu
·
You can use other
microphones with SpeechViewer III but the Shure model that is packaged is a
high quality model that will ensure accuracy and guarantee success. You can
turn the microphone on or off by using a menu item (Settings/ Microphone/
Delete) or use the switch on the neck of the microphone itself. There is a Too
Loud Threshold where you can increase or decrease the loudness (as some clients
may speak too loudly). Reinforcements are the “fireworks” or visual and
auditory rewards that go off when a client completes an exercise. You can
choose from None, Graphics and Sound or Graphics Only.
The Phoneme List has only one choice i.e. English (phonics). The System Time
shows your computer’s date and time settings. Notes and files are date stamped
according to your computer’s settings.
The Actions Menu
· Choose New Graphic displays a new landscape for your exercise. Play Back allows you to listen to the last eight seconds of speech/sound made by the client. Display Statistics shows the data that has been collected for the current exercise where Reset Statistics clears the currently collected statistics.
· SpeechViewer III is a complete tool that has a number of motivating and captivating phoneme exercises that you use with a personalised phoneme model file. It offers a powerful set of exercises by offering entertaining game formats that invite participation from clients of all ages. Speech/language pathologists, teachers, parents and other professionals use it to modify speech patterns.
2.2 Use of computer based speech equipment for management of voice in children with hearing impairment
Profoundly hearing-impaired children often suffer from disorders of physiological control like deviant respiratory patterns as well as breathiness, voice breaks, unstable pitch, nasality and vocal fry. This is due to a restricted use of the vocal apparatus and the fact that they have to learn oral language by a laborious visual imitation of speaking (Grewel, 1963). Non-visible speech elements like for instance, nasality, voicing, and fundamental frequency can be related to typical deviations in the speech of profoundly hearing-impaired children.
Nasalance Module
In this module, the speech output from the lips (oral level) as well as the nostrils (nasal level) is broadly separated and their respective levels are measured. Thus one can become aware of the level of the speech output coming from the nostrils and lips separately. For example, when a word like ‘appa’ if said properly, has no nasalance. On the other hand, when a word like ‘amma’ is said properly, there will be a presence of a nasal sound in the word. The colourful display of the levels in this module helps even a hard of hearing client to become aware of the production of nasal sounds.
Nasalence Measurement
When Nasalence is measured quantitatively, for an ideal voice, for steady vowels, the nasalence must be 0%; In case of ‘hyper-nasality’, if the problem is due to lack of awareness, rather than an organic disorder, therapy is your solution.
Ideally, when pronouncing ‘m’ or ‘n’, nasalence must be as high as possible (>80%). If not, the case is called ‘hypo-nasality’ and can be corrected using therapy if the problem is due to lack of awareness, rather than any organic disorder.
The unique feature of the various modules developed by Voice and Speech Systems is that it not only provides therapy for various and numerous dimensions of voice and speech problems but it also gives you an option to measure your deviation from the normal. Using Vagmi Therapy Nasalence Module one can not only correct hyper or hypo nasality by means of interesting games but also first measure the degree of deviation from the normal voice quality and the severity of nasalence in one’s voice.
There is an organ called ‘velum’ near the root of the tongue. Sometimes this is referred to as ‘little tongue’. This acts as a valve. Lifting this valve leads to the blockage of sounds via the nostrils producing a nasal voice. On the other hand, this valve or the velum has to be lowered to produce sounds such as ‘m’, ‘n’. When a person is unable to control the movement of velum and if it is always in a lowered position then his/her speech sounds highly nasal. This is called ‘nasal voice’.
The inability to move the velum may be because of lack of awareness or bad practice. In such a case therapy programs help one become aware of the action of velum and there by learn to regulate it. On the other hand, if the nerve connecting to the muscles of the velum is unable to activate it, it is a permanent damage, may be since birth – a congenital defect. In such a case therapy will not help.
Therapy for Breath Support Module
The duration for which a client is able to say a steady vowel with a single breath is referred to as the maximum phonation duration (MPD) or maximum phonation time (MPT). Poor MPD may arise either because of poor respiratory support or inefficient use of the available air in the lungs.
Vagmi Therapy Breath Support Module gives you Measurement or Assessment as well as Therapy menu options to help increase breath support such that the client is able to talk with strength in their voice and for longer duration without getting tired.
· Voice Initiation and Sustenance– This is a measurement program to verify if the client’s voice has sufficient respiratory support.
· MPD Measurement – This is to measure the MPD as well as to check the steadiness in the client’s voice.
· MPD Therapy – This has a number of games like Pacman, puzzles and many challenges to help the client increase their breath support to be able to talk for a long duration comfortably.
Therapy for Voice Control Module
If voice is of breathy quality, a qualified speech language pathologist or ENT specialist can ascertain this using the menu options ‘Acoustic Glottogram’ for measurement and ‘Glottal Leakage for therapy.
Acoustic Glottogram
The phonation signal of a steady ‘aa’ or ‘A’ is recorded and the air flow through the glottis is deduced. The ‘pattern’ or the ‘shape’ of the air flow through the glottis depends on the manner of vibration of the vocal folds. Thus an experienced professional can interpret the voice quality as breathy or modal or pressed or falsetto by looking at this pattern. Also, the opening, closing and closed durations relative to pitch period can be deduced. Using the pattern displayed as a feedback, the client may try to improve the voice quality.
Glottal Leakage
The duration for which a client can say a steady vowel with a single breath is referred to as the maximum phonation duration (MPD). Although the respiratory support of the client is good, the air stored in the lungs may be depleted very fast due to the client’s breathy voice. This module provides a graphic display corresponding to the voice quality of the client. One has to achieve as large a phonation duration as possible while maintaining a good voice quality.
Voice Focus
The pronunciation of sounds must be clearly enunciated. If the movement of the articulatorstongue, jaw and lips is highly restricted then the voice quality is poor. Examples of poor voice quality are ‘clenched teeth’, ‘palatalized’ etc. The client is asked to say steady vowels or vowels in a context. Then, the module measures and gives a graphic display of the spread in ‘vowel space’. When the vowel space of the client is compared with the vowel space of a normal reference, it gives an idea about how clustered or blurred one’s voice is for correction.
2.3 Use of computer based speech equipment for management of suprasegmental features of speech in children with hearing impairment
So far all the sounds we’ve been considering are segments: the individual speech sounds that we represent with IPA symbols. But when we speak, we also include sounds that are above or beyond the level of the segments. This sound information is called prosody, or suprasegmental information, and it makes up the rhythm, timing, meter, and stress of the words and sentences that we speak. The primary pieces of suprasegmental information are the pitch of sounds, the loudness, and the length.
The pitch of a sound is how high or low it is. We produce high pitched sounds when our vocal folds have a high-frequency vibration, and when our vocal folds vibrate more slowly, the resulting sound is lower in pitch.
Some languages use pitch information to signal changes in word meaning. If a language uses pitch this way, the pitch information is called tone. These example words are from Yoruba, a language spoken in Nigeria. If you look just at the segmental level, these words all seem to be transcribed the same. But speakers of Yoruba vary their pitch when they speak these words so that the meaning of the word changes depending on whether the second syllable has a high tone, a mid-tone, or a low tone. Probably the best-known tone language is Mandarin, which has five different tones. Looking at these five words, you can see that they contain the same segments, but it’s the tones that distinguish their meaning.
Languages also use pitch in another way, not to change word meaning, but to signal information at the level of the discourse, or to signal a speaker’s emotion or attitude. When pitch is used this way, it’s called intonation rather than tone. English uses pitch for intonation — let’s look at some examples.
Sam got an A in Calculus.
Sam got an A in Calculus!
Sam got an A in Calculus?
Sam? got an A? in Calculus?
All of these sentences contain the same words (and the same segments) but if we vary the intonation, we convey something different about the speaker’s attitude towards the sentence’s meaning. Notice that we sometimes use punctuation in our writing to give some clues about a sentence’s prosody.
Another component of suprasegmental information is the length of sounds. Some sounds are longer than others. Listen carefully to these two words in English. beat, bead. The vowel sound in both words is the high front tense vowel [i]. But in bead, the vowel is a little longer. This is a predictable process in English — vowels get longer when there’s a voiced sound in the coda of the syllable. The diacritic to indicate that a segment is long looks a bit like a colon [iː].
So a sound can change in length as the result of a predictable articulatory process, or, like intonation, length can signal discourse-level information about an utterance. Consider the difference between, That test was easy, and, That test was eeeeeeeeeeeeeaaasyyyyyyyy. Some languages use length contrastively, that is, to change the meaning of a word. In these words in Yapese, a language of the Western Pacific region, you can see that making a vowel long leads to a completely different word with a new meaning. In these words from Italian, consonant length can change the meaning of a word, so fato means fate, but fatto means fact.
To sum up, suprasegmental information, also known as prosody, is that sound information that’s above the level of the segment. It consists of pitch, loudness, and length. Many languages use prosody to provide discourse-level information, and some languages also use prosody to change word meanings.
Suprasegmental Aspects of Speech
Syllables
· Prominence
· Parts of syllable - onset, coda, nucleus rhyme
· Stress
· Contrastive stress
· Lexical stress
· Degrees of stress?
· Stress in sentences
Intonation and pitch
· Pitch changes within phrase
· Tonic accent
· Tone language
Children with hearing impairment have been found to have a monotonous rhythm due to incorrect pausing between syllables. Sometimes their fundamental frequency is extremely high with a lowering at the end of every vowel. The children also had extended segment duration.
Children with a normal speaking rate however may not have fluent speech fluent, due to the fact that they breathe after every second word. They may emphasize the beginning and the end of every sentence. The most interesting deviation is vowel-dependent fundamental frequency variation because of an excessive articulatory tension. Some children might have a normal fundamental frequency but a remarkably slow tempo. Furthermore, they might as well extend the occlusion phase in the production of the plosives /p, t, k/. The prosodic deviations of each child forms the basis for the rules used to generate the prosody of the simulated speech.
Computer-based speech pronunciation teaching systems generally include measuring and displaying the dynamic characteristics of speech parameters, using auditive, visual and automatic feedback.
The following module is usually incorporated for management of suprasegmentals:
Intonation and Accent Module
Intonation
The variation in pitch over the length of an utterance is measured while a client speaks and it is determined if the client’s voice has some intonation or is dull, flat or monotone. By testing the steadiness in voice, this module also helps as a preliminary screening tool of a voice disorder. This feature can also be used for practicing to sing a musical note at a particular appropriate pitch. Also, the same program may be used to measure the range of pitch– lowest to highest. By displaying the volume instead of the pitch, rhythmic patterns of short and long vowels in syllables also may be displayed.
Accent
This feature is language independent. A model utterance of any language can be recorded and saved. This model intonation pattern to be achieved can be displayed in the upper window. The intonation of the client’s production is shown in the lower window for comparison to achieve the desired intonation of the chosen language. The client can also listen to the model utterance and compare it with his/her own production thus getting close and achieving the desired intonation pattern.
2.4 Basic infrastructure required for using computer based speech training aids/equipment
The terms equipment and infrastructure in this chapter refer to computer hardware and associated communications equipment and cabling, as well as other technology-related equipment regularly used in schools. Indicators address the availability, capabilities, and connectivity of computer equipment and infrastructure.
Computer equipment refers to both computers and associated peripheral equipment, such as:
- computers, including desktop and laptop machines, but extending to handheld computers (also known as Personal Digital Assistants, or PDAs), mainframe machines, and other specialized computing devices; and
- peripheral equipment that may be attached to computers, such as monitors, keyboards, disk drives, modems, printers, scanners, cameras, and speakers.
Other technology resources in the school setting are also included, such as:
- network devices-routers, hubs, switches, access servers;
- communications support, such as fax-back and voice-mail resources in regular use by instructional and administrative staff;
- videoconferencing and other distance education tools, including satellite transmitters and receivers, cable-based receivers, and modem or codec-based video equipment;
- projection devices, from transparent and opaque projectors to video monitors; and
- graphing calculators and other specialized computational aids.
The term infrastructure covers both devices and cabling. Devices supporting technology in schools include specialized equipment (such as switches, routers, modems, or codecs) that link computers or video hardware to networks. Infrastructure also refers to cabling, whether wire, fiber optic, or coaxial. In newer systems, links between computers are wireless, in which case infrastructure refers to receivers and transmitters.
For schools to use technology, they must first have it and make it available for students, teachers, and administrative staff. Acquiring that technology, from computers to modems to two-way conferencing equipment, is only one step in facilitating student learning. Curriculum integration and professional development are also essential components in this process.
Room and equipment:
For an effective computer based speech training it is pertinent to have a few stringent criterions. According to Rehabilitation council of India guidelines an institute with speech science lab should ideally be a quiet room. The average size of the room should be (6*6) sq. ft.. With computer PC- AT with VGA color monitor. Hi- fi ampli deck with speakers and good microphone, software for diagnostic/therapeutic use, audio cassettes for training. Other important factors to be considered are a well lit room with good aeration. Comfortable seating arrangement and a less reverberant room is desirable. The cleanliness of the room and equipment is essential. Power cables should be nicely secured. A power back up with voltage stabilizer is also required for unobstructed training program.
Speech training system:
What distinguishes a good computer-based speech training system? Throughout the literature many design considerations are mentioned, but few are collected into a theoretical framework against which different systems can be compared or analyzed.
Watson and Kewley-Port (1989) argues that a good system should possess the same properties as a speech therapist and defines this with the following characteristics;
· being able to assess the speech of a child and distinguish problem areas, being able to make a treatment plan
· Give cues in form of produced speech; give feedback based on the child’s production and keep records of how the child performs.
· physical source of feedback, from which modality is the information of the speech production obtained, standards of evaluation, what kind of model should be used to compare the speech production with and level and type of detail on which feedback is based, that is how much processing should be done before the result is displayed and in which form it should be displayed.
Mahshie (1995) also carries out a discussion on good computer-based aids and does this from three main pedagogical factors. The task and target skills the child needs to learn, the cues given to the child and the feedback on how good the production was. Interesting here is perhaps the task and target skill that is not mentioned by Watson and Kewley-Port. Other important considerations mentioned in the literature are those concerned with most computer-based systems. The system must be easy to use, clear instructions are needed and, the system must be acceptable for both therapists and children (Oster 1996).
· Clear instructions and pedagogical manuals must be created and made available for use with different groups of children.
· The visual feedback of the child’s voice and articulation should be shown immediately and without delay.
· The aid must be acceptable to the therapist as well as to the child, which means that the aid must be attractive, interesting, easily comprehensible, easy to handle, and motivating.
· The visual pattern must be natural, logical and easily understandable. This means that training parameters as, e.g., pitch could be shown vertically as pitch variations occur; intensity through the size of an object that becomes larger as a sound becomes louder and smaller as a sound becomes softer; intonation and stress through a continuous red curve; duration could be shown horizontally and voicing through a relationship between voicing and the change of a color.
· The aid should provide a contrastive training, that is, the correct model of the therapist and the deviant production of the child are shown simultaneously and compared with each other.
· The aid should provide a flexible, individual, and structural speech and voice training and give an objective evaluation of the child’s training results.
2.5 Tele Speech Therapy
Teletherapy is the provision of therapy based healthcare services remotely through telecommunication technology. Therapy practitioners have utilized electronic communication to provide therapy services in recent years. They may refer to such service provisions as teletherapy, telerehab, or telemedicine.
Therapy services available through telecommunication include speech therapy, occupational therapy, and physical therapy services.
OPERATIONAL DEFINITIONS:
1. Telepractice (with reference to ASLP- AUDIOLOGY AND SPEECH, LANGUAGE PATHOLOGY): Telepractice is the provision of ICT based clinical services including screening, diagnostic and rehabilitative services in audiology and speech, language pathology by a professional
2. Professional : Audiologist or Speech-language Pathologist with minimum qualification of undergraduate degree in audiology and speech-language pathology, registered with RCI, who engages in providing ICT based clinical services
3. Facilitator: Personnel available at the client’s location to assist the professional in delivering appropriate clinical services remotely. Facilitator executes their roles and responsibilities only under the guidance and supervision of a qualified professional.
4. Client: Recipients of ASLP services through telepractice
Tele Speech Therapy /Telepractice is the application of telecommunications technology to the delivery of speech language pathology and audiology professional services at a distance by linking clinician to client/patient or clinician to clinician for assessment, intervention, and/or consultation. Supervision, mentoring, and pre-service and continuing education are other activities that may be conducted through the use of technology.
Tele-speech therapy is the use of telecommunication technology to connect the therapist with the patient. In the case of Speech Therapy, the therapist can conduct a proper therapy session. Both the therapist and the patient need a computer with a webcam and a good internet signal. With Teletherapy the distance between the patient and the therapist is immaterial. It could be a few kilometers or a few thousand kilometers.
The volume of searches on Google for “Speech Therapy near me” or “Speech Therapy Centre near me” and “Speech Therapy at home” indicate that people are interested in a Speech Therapist close by.
Types of Tele speech therapy
The two most common terms describing types of telepractice are synchronous (client/patient interactive) and asynchronous (store and forward).
- Synchronous—Services are conducted with real-time audio and/or video connection to create an experience similar to that achieved in an in-person traditional encounter. Synchronous services may include, for example, connecting a client or a group of clients with a clinician, or they may include consultation between a clinician and a specialist. Telehealth visits, virtual check-ins, e-visits, or virtual consultations are examples of synchronous services.
- Asynchronous—Information, images, video, or data are saved and transmitted for viewing or interpretation at a later time. Examples include transmission of voice clips, audiologic testing results, patient education materials, or outcomes of independent client practice. Store-and-forward or chat-based interactions are examples of asynchronous services.
- Hybrid—A combination of synchronous, asynchronous, remote patient monitoring (e.g., wearable sensors, mobile apps), and/or in-person services are implemented to meet the needs of the individual client. An example includes using an online or a mobile app to share asynchronous information between the client and the clinician between synchronous in-person or virtual sessions.
Tools for telepractice
i. Computers/mobile phones/ tablets: Telecommunication devices such as laptop/ desktop computers, smartphones and tablets along with its peripherals may be used for telepractice. The professional must ensure appropriate selection of devices based on client needs, clinical service requirements and test equipment to be connected. These devices must be routinely checked for optimum functioning.
ii. Telecommunication platform
a) Video conferencing software: Video conferencing can be accomplished using desktop or cloud-based software and dedicated videoconferencing hardware systems. It is recommended to use videoconferencing software that explicitly provides details regarding data encryption and data protection and privacy. Platforms available in public domain including Google hangouts/ Skype/Facetime/WhatsApp should be used with caution as encryption of data is not explicitly known and therefore does not ensure patient data privacy.
Selection of videoconferencing platform should be based on the bandwidth requirements, storage capacity of the device to be used, user friendliness (for both professional and client) of the software interface, number of hosts and attendees permitted (in case of group therapy sessions etc.), and privacy/security features. Features such as screen sharing; whiteboard; unlimited video calls, file sharing, chat box; recording and interactivity features (e.g., animations, stamps) are desirable. Videoconferencing peripherals include camera with good resolution, display monitor, headsets, microphone and speakers.
b) Text messaging/Emails: Text messaging and emails may be used for exchanging information and resources that supports the client’s clinical needs
c) Remote computing software: Remote computing/ desktop software is a tool that uses virtual network computing (VNC) to allow one computer to remotely access and control another computer over an internet/network connection. These software are particularly required to control test equipment that are connected to a computer and controlled by software (E.g. Audiometer, ABR, OAE). There are standalone remote computing software such as RemotePC, Remote Desktop Manager, and there are some videoconferencing software which also have remote computing capability such as Teamviewer etc. It is recommended to use remote computing software that explicitly provides details regarding data encryption and data protection and privacy.
iii. Connectivity:
Telecommunication link between the professional and client site is established through internet connectivity. ISDN, DSL, cable, fibre optic and satellite are different sources of internet connectivity. Each of these options have their strengths and limitations with respect to bandwidth and speed, cost and coverage. Network connection speed affects overall quality of video and audio clarity. Higher bandwidth is required for real-time testing or videoconferencing. Lower bandwidth may result in lags, disrupted voice and video quality. Method of telepractice (stated below under section 4) should be chosen by the professional based on availability of internet bandwidth and speed at professional site and clientsite.
iv. Test equipment/tools: Telepractice may involve testing equipment to be available at client site. Audiological services are particularly equipment intensive with use of computer based audiometers, Immittance, OAE, ABR etc. There may also be other peripheral devices, such as recording devices or auxiliary video input equipment for computer interfacing, document cameras, or other specialized cameras with high resolution (e.g., fiberoptic videoendoscopes) Reasonable care should be exercised when selecting equipment for evaluating or treating a client. Since these equipment will be handled by the facilitator at the client site, it is important that the equipment is sturdy, easy to use and compact. Wherever applicable, equipment specialised for tele-practice maybe used for optimum testing. Professionals must be fully aware of the capabilities and limitations of the equipment they intend to use, and the impact it may have on service delivery.
Mobile phone/tablet based apps that are primarily meant for screening of hearing or speech-language should not be used as diagnostic or confirmatory tests. When such apps are used for screening, the professional should verify white papers related to the validity of the app or must validate the app before using it for clinical purposes.
Diagnosis should be made only based on uncompromised standard test protocoI. Recommendations for rehabilitation cannot be based on results obtained using screening apps.
Issuance of disability certification to a client using telepractice should be based on standard test procedures for certification purposes and with prior approval of such a methodology by the concerned government authority.
v. Adaptations of test materials for assessment and rehabilitation:
Delivery of services via telepractice, may require modifications to treatment material. Assessment and therapy materials/ tools must be available in digital format. Materials used in the telepractice session must be adapted to suit needs of persons with disabilities. Validated apps available for speech-language therapy, aural rehabilitation, tinnitus management etc. could be used for clients as per requirement. However, such app based therapeutic interventions must be supervised by the professional. The professional should use apps which are culturally and linguistically appropriate for Indian population.
Rules and Regulations of Telepractice:
· Individuals who hold the degree in Speech language Pathology and audiology should be trained in telepractising can only perform this service.
· Professionals shall evaluate the effectiveness of services provided, technology employed, and products dispensed, and they shall provide services or dispense products only when benefit can reasonably be expected.
· Individuals shall make use of technology and instrumentation consistent with accepted professional guidelines in their areas of practice. When such technology is not available, an appropriate referral may be made.
· Individuals shall ensure that all technology and instrumentation used to provide services or to conduct research and scholarly activities are in proper working order and are properly calibrated.
Roles and responsibilities for audiologists and SLPs in the provision of services via telepractice include
· understanding and applying appropriate models of technology used to deliver services;
· understanding the appropriate specifications and operations of technology used in delivery of services;
· calibrating and maintaining clinical instruments and telehealth equipment;
· selecting clients who are appropriate for assessment and intervention services via telepractice;
· selecting and using assessments and interventions that are appropriate to the technology being used and that take into consideration client/patient and disorder variables;
· being sensitive to cultural and linguistic variables that affect the identification, assessment, treatment and management of communication disorders/differences in individuals receiving services via telepractice;
· training and using support personnel appropriately when delivering services;
· being familiar with the available tools and methods and applying
· maintaining appropriate documentation, including informed consent for use of telepractice and documentation of the telepractice encounter;
· being knowledgeable and compliant with existing rules and regulations regarding telepractice including security and privacy protections, reimbursement for services, and licensure, liability and malpractice concerns;
· collaborating with physicians for timely referral and follow-up services (Hofstetter, Kokesh, Ferguson, & Hood, 2010);
· using web-based technology to engage clients through virtual environments and other personally salient activities (Towey, 2012).
Telepractice is constantly evolving. Ongoing education and training is required to maintain expertise and familiarity with changes in technology and potential clinical applications.ng them to evaluate the effectiveness of services provided and to measure outcomes;
Key benefits of teletherapy
Convenience: Teletherapy offers the ultimate convenience. Parents and children can receive therapy from the comfort of their own home, which eliminates the need to pack up and travel to a clinic. It also means that families can access therapy from home without feeling the need to clean up or put on shoes.
Motivating Technology: Children are naturally drawn to technology, and teletherapy is no exception. The interactive platform, games, and comprehensive evaluations provided by the therapist keep children motivated and engaged throughout the session. With teletherapy, children are given the opportunity to use technology for a productive purpose, making it an effective and engaging approach to therapy.
Access to Highly Specialized Therapists: Teletherapy offers access to specialized treatment approaches and clinicians that are not available in certain areas. For instance, if you are in a rural area and do not have easy access to therapy, you can now receive therapy in the comfort of your home. Additionally, for those who require a specialized treatment approach, teletherapy can offer your child a clinician that has the right expertise and training.
Opportunity for Parent or Caregiver Involvement: Another one of the benefits of therapy at home is the opportunity to be more involved in your child’s therapy sessions. If your child is older, and independently participating in teletherapy, you will have the opportunity to meet with your therapist before or after each session. For younger children or those that require more support, you will have the opportunity to learn and apply therapy strategies during and after each session. These therapy strategies can often be integrated into your routine and practiced throughout your week.
Teletherapy is a convenient, and effective method of service delivery. With the added perks of accessibility, specialized treatment approaches, children’s love of technology, and the opportunity for parent and caregiver involvement, it’s no wonder why teletherapy has become increasingly popular.