INTRODUCTION
Hearing impairment is a partial or total inability to hear. It is a disability which is sub-divided in two categories of deaf and hard of hearing.
- “Deaf” means persons having 70 dB hearing loss in speech frequencies in both ears.
- “Hard of hearing” means person having 60 dB to 70 dB hearing loss in speech frequencies in both ears.
A pure tone audiometry test measures the softest, or least audible, sound that a person can hear. During the test, you will wear earphones and hear a range of sounds directed to one ear at a time. The loudness of sound is measured in decibels (dB).
Person with disability act- (PWD, 1995)
· Definition of disability in pwd act includes hearing impairment- Hearing impairment means loss of 60 decibel or more in the better ear in speech conversation frequencies.
Centre for diseases control and prevention (CDC) – Refers to hearing impairment as conditions that affect the frequency and or intensity of one’s hearing. Individuals with mild to moderate hearing impairments may be “hard of hearing” but are not “deaf” these individuals differ from deaf individuals as they use their hearing to assist in communication with others
CLASSIFICATION
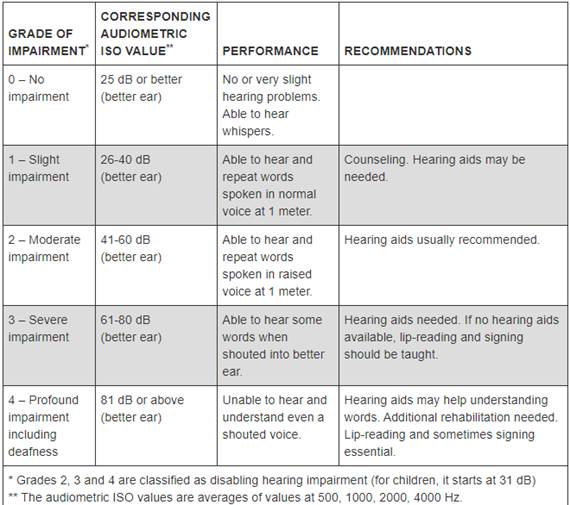
According to degree of impairment – WHO
According to place of impairment –
· Conductive hearing loss – hearing loss due to the interference in the transmission of sound to and through the sense organ (outer or middle ear). Conductive hearing loss can be caused by blockage of the external canal, perforation of the eardrum, infections and diseases of the middle ear, and disruption or fixation of the small hearing bones. A person with a conductive hearing loss may hear better in noise than in quiet and generally hears well over the telephone. Total deafness is rarely the result of conductive hearing impairments, and a properly fitted hearing aid usually provides benefit. Sometimes a surgical correction can improve the hearing.
· Sensory-neural hearing loss – due to the abnormality of the inner ear or the auditory nerve, or both. Sensorineural hearing impairment is more common and has many possible causes. Usually the condition results in slow, gradual loss of the sound receptors and nerve endings. Patients may experience a lack of sensitivity to sound or a lack of interpretation or clarity of sound. Speech understanding is difficult when there is background noise, and hearing sensitivity is usually better for low tones than high-pitched sounds. Hearing aids provide benefit for many patients with sensorineural impairment by amplifying sounds. However hearing aids typically do not increase the clarity of speech. When speech understanding deteriorates significantly, hearing aids may not provide sufficient benefit. Many of such patients are good candidates for a cochlear implant. These devices are surgically implanted and directly stimulate the hearing nerve to improve the ability to hear sounds and the ability to understand speech.
· Mixed hearing loss - combination of both; sometimes called a flat loss. This is a combination of conductive and sensorineural hearing loss. Long-term ear infections can damage both the eardrum and the ossicles. Sometimes, surgical intervention may restore hearing, but it is not always effective.
According to the age at onset of deafness
• Congenitally deaf – born deaf
• Adventitiously deaf – born with normal hearing and became deaf through accident/illness
According to language development-
• Pre-lingually deaf – born deaf or lost hearing before speech and language were developed
• Post-lingually deaf- lost hearing after development of spontaneous speech and language
CAUSES
The causes of hearing loss and deafness can be congenital or acquired.
Congenital causes
Congenital causes may lead to hearing loss being present at or acquired soon after birth. Hearing loss can be caused by hereditary and non-hereditary genetic factors or by certain complications during pregnancy and childbirth, including:
- maternal rubella, syphilis or certain other infections during pregnancy;
- low birth weight;
- birth asphyxia (a lack of oxygen at the time of birth);
- inappropriate use of particular drugs during pregnancy, such as aminoglycosides, cytotoxic drugs, antimalarial drugs, and diuretics;
- severe jaundice in the neonatal period, which can damage the hearing nerve in a newborn infant.
Acquired causes
Acquired causes may lead to hearing loss at any age, such as:
- infectious diseases including meningitis, measles and mumps;
- chronic ear infections;
- collection of fluid in the ear (otitis media);
- use of certain medicines, such as those used in the treatment of neonatal infections, malaria, drug-resistant tuberculosis, and cancers;
- injury to the head or ear;
- excessive noise, including occupational noise such as that from machinery and explosions;
- recreational exposure to loud sounds such as that from use of personal audio devices at high volumes and for prolonged periods of time and regular attendance at concerts, nightclubs, bars and sporting events;
- ageing, in particular due to degeneration of sensory cells; and
- wax or foreign bodies blocking the ear canal.
Among children, chronic otitis media is a common cause of hearing loss.
RISK
Factors that may damage or lead to loss of the hairs and nerve cells in your inner ear include:
· Aging. Degeneration of inner ear structures occurs over time.
· Loud noise. Exposure to loud sounds can damage the cells of your inner ear. Damage can occur with long-term exposure to loud noises, or from a short blast of noise, such as from a gunshot.
· Heredity. Your genetic makeup may make you more susceptible to ear damage from sound or deterioration from aging.
· Occupational noises. Jobs where loud noise is a regular part of the working environment, such as farming, construction or factory work, can lead to damage inside your ear.
· Recreational noises. Exposure to explosive noises, such as from firearms and jet engines, can cause immediate, permanent hearing loss. Other recreational activities with dangerously high noise levels include snowmobiling, motorcycling, carpentry or listening to loud music.
· Some medications. Drugs such as the antibiotic gentamicin, sildenafil (Viagra) and certain chemotherapy drugs, can damage the inner ear. Temporary effects on your hearing — ringing in the ear (tinnitus) or hearing loss — can occur if you take very high doses of aspirin, other pain relievers, antimalarial drugs or loop diuretics.
· Some illnesses. Diseases or illnesses that result in high fever, such as meningitis, may damage the cochlea.
PREVENTION
Some simple strategies for prevention of hearing loss include:
- immunizing children against childhood diseases, including measles, meningitis, rubella and mumps;
- immunizing adolescent girls and women of reproductive age against rubella before pregnancy;
- preventing cytomegalovirus infections in expectant mothers through good hygiene; screening for and treating syphilis and other infections in pregnant women;
- strengthening maternal and child health programmes, including promotion of safe childbirth;
- following healthy ear care practices;
- reducing exposure (both occupational and recreational) to loud sounds by raising awareness about the risks; developing and enforcing relevant legislation; and encouraging individuals to use personal protective devices such as earplugs and noise-cancelling earphones and headphones.
- screening of children for otitis media, followed by appropriate medical or surgical interventions;
- avoiding the use of particular drugs which may be harmful to hearing, unless prescribed and monitored by a qualified physician;
- referring infants at high risk, such as those with a family history of deafness or those born with low birth weight, birth asphyxia, jaundice or meningitis, for early assessment of hearing, to ensure prompt diagnosis and appropriate management, as required;
- implementing the WHO-ITU global standard for personal audio systems and devices. This can be done by governments and manufacturers of smartphones and MP3 players. If adhered to, the standard could help prevent hearing loss due to listening practices that are harmful to hearing; and
- educating young people and population in general on hearing loss, its causes, prevention and identification.
DIAGNOSIS
Measurement of Air Conduction Thresholds (ACT)
1. ACT is to be measured using standard Pure Tone Audiometry by an Audiologist for Right Ear and Left Ear separately
2. In case of non-reliable ACT, additional tests are recommended such as Immittance, and Speech audiometry or Auditory Brainstem Response (ABR) Testing
3. Measuring ACT may be difficult in children aged 3-5 years. In such cases, Conditioned Pure Tone audiometry/Visual Reinforcement Audiometry (VRA) shall be conducted. ABR or Auditory Steady State Response (ASSR) testing can be advised for the estimation of ACT in infant and young children
Computation of Percentage of Hearing Disability
1. Calculate Pure tone average of ACT for 500 Hz, 1000 Hz, 2000 Hz, 4000 Hz for Right Ear and Left ear separately (whenever there is no response at any frequency ACT is to be considered as 95dB)
2. Monaural percentage of hearing disability is to be calculated as per the ready reckoner separately for Right Ear and Left Ear
Formula for Calculating Percentage of Hearing Disability
Percentage of Hearing Disability = (Better ear % of hearing disability x 5) + (Poorer ear % of hearing disability) / 6
A tuning fork test: This is also known as the Rinne test. A tuning fork is a metal instrument with two prongs that produces a sound when it is struck. Simple tuning fork tests may help the doctor detect whether there is any hearing loss, and where the problem is.
A tuning fork is vibrated and placed against the mastoid bone behind the ear. The patient is asked to indicate when they no longer hear any sound. The fork, which is still vibrating, is then placed 1 to 2 centimeters (cm) from the auditory canal. The patient is asked again whether they can hear the fork.
As air conduction is greater than bone conduction, the patient should be able to hear the vibration. If they cannot hear it at this point, it means that their bone conduction is superior to their air conduction.
This suggests a problem with sound waves getting to the cochlea through the ear canal.
Audiometer test: The patient wears earphones, and sounds are directed into one ear at a time. A range of sounds is presented to the patient at various tones. The patient has to signal each time a sound is heard.
Each tone is presented at various volumes, so that the audiologist can determine at which point the sound at that tone is no longer detected. The same test is carried out with words. The audiologist presents words at various tones and decibel levels to determine where the ability to hear stops.
Bone oscillator test: This is used to find out how well vibrations pass through the ossicles. A bone oscillator is placed against the mastoid. The aim is to gauge the function of the nerve that carries these signals to the brain.
TREATMENT
Help is available for people with all types of hearing loss. Treatment depends on both the cause and severity of the deafness.
Sensorineural hearing loss is incurable. When the hair cells in the cochlea are damaged, they cannot be repaired. However, various treatments and strategies can help improve quality of life.
Hearing aid:
Hearing aids can help to improve hearing and quality of life. These are wearable devices that assist hearing.
There are several types of hearing aid. They come in a range of sizes, circuitries, and levels of power. Hearing aids do not cure deafness but amplify the sound that enters the ear so that the listener can hear more clearly. Hearing aids consist of a battery, loudspeaker, amplifier, and microphone. Today, they are very small, discreet, and can fit inside the ear. Many modern versions can distinguish background noise from foreground sounds, such as speech.
A hearing aid is not suitable for a person with profound deafness. The audiologist takes an impression of the ear to make sure the device fits well. It will be adjusted to suit auditory requirements.
Examples of hearing aids include:
Behind-the-ear (BTE) hearing aids: These consist of a dome called an earmold and a case, with a connection linking one to the other. The case sits behind the outer ear, with the connection to the dome coming down the front of the ear. The sound from the device is either electrically or acoustically routed to the ear.
BTE hearing aids tend to last longer than other devices, as the electrical components are located outside the ear, meaning that there is less moisture and earwax damage These devices are more popular with children who need a sturdy and easy-to-use device.
In-the-canal (ITC) hearing aids: These fill the outer part of the ear canal and can be seen. Soft ear inserts, usually made of silicone, are used to position the loudspeaker inside the ear. These devices fit most patients straight away and have better sound quality.
Completely in the canal (CIC) hearing aids: These are tiny, discreet devices but not recommended for people with severe hearing loss.
Bone conduction hearing aids: These assist people with conductive hearing loss, as well as those unable to wear conventional type hearing aids. The vibrating part of the device is held against the mastoid with a headband. The vibrations go through the mastoid bone, to the cochlea. These devices can be painful or uncomfortable if worn for too long.
Cochlear implants:
If the eardrum and middle ear are functioning correctly, a person may benefit from a cochlear implant.
This thin electrode is inserted into the cochlea. It stimulates electricity through a tiny microprocessor placed under the skin behind the ear.
A cochlear implant is inserted to help patients whose hearing impairment is caused by hair cell damage in the cochlea. The implants usually improve speech comprehension. The latest cochlear implants have new technology that helps patients enjoy music, understand speech better even with background noise, and use their processors while they are swimming.
On the outside, a cochlear implant consists of:
- A microphone: This gathers sound from the environment.
- A speech processor: This prioritizes the sounds that matter more to the patient, such as speech. The electrical sound signals are split into channels and sent through a very thin wire to the transmitter.
- A transmitter: This is a coil secured with a magnet. It is located behind the outer ear and transmits the processed sound signals to the internally implanted device.
On the inside:
- A surgeon secures a receiver and stimulator in the bone beneath the skin. The signals are converted into electrical impulses and sent through internal wires to the electrodes.
- Up to 22 electrodes are wound through the cochlea. The impulses are sent to the nerves in the lower passages of the cochlea and then directly to the brain. The number of electrodes depends on manufacturers of the implant.
Children will usually have cochlear implants in both ears, while adults tend to have just one.